You might also like
- Blurred Vision Headache: Hyperopia Myopia AstigmatismDocument4 pagesBlurred Vision Headache: Hyperopia Myopia Astigmatismraquel maniego100% (1)
- TEST II Community Health Nursing and Care of The Mother and Child XDDocument11 pagesTEST II Community Health Nursing and Care of The Mother and Child XDraquel maniegoNo ratings yet
- Cancer BulletsDocument3 pagesCancer Bulletsraquel maniegoNo ratings yet
- DCIS: The Treatment Debate: Lesley Street Advisor: Dr. HadleyDocument15 pagesDCIS: The Treatment Debate: Lesley Street Advisor: Dr. Hadleyraquel maniegoNo ratings yet
- TEST I - Foundation of Professional Nursing PracticeDocument11 pagesTEST I - Foundation of Professional Nursing Practiceraquel maniegoNo ratings yet
- Nclex Exam Maternal and Child Health Nursing 1 30 ItemsDocument7 pagesNclex Exam Maternal and Child Health Nursing 1 30 Itemsraquel maniegoNo ratings yet
- TanDocument23 pagesTanraquel maniegoNo ratings yet
- Minor Body Changes of PregnancyDocument41 pagesMinor Body Changes of Pregnancyraquel maniegoNo ratings yet
- Ob Final ReviewDocument13 pagesOb Final Reviewraquel maniegoNo ratings yet
- Summary Rizal Chap 7Document12 pagesSummary Rizal Chap 7raquel maniegoNo ratings yet
- Summary Complete Mental Health NursingDocument20 pagesSummary Complete Mental Health Nursingraquel maniegoNo ratings yet
- Pediatric Asthma WordDocument4 pagesPediatric Asthma Wordraquel maniegoNo ratings yet
- Anatomy and Physiology of The Spine: Google ImagesDocument9 pagesAnatomy and Physiology of The Spine: Google Imagesraquel maniegoNo ratings yet
- Therapeutic CommunicationDocument6 pagesTherapeutic Communicationraquel maniegoNo ratings yet
- Post Operative CareDocument4 pagesPost Operative Careraquel maniegoNo ratings yet
- PharmacologyDocument7 pagesPharmacologyraquel maniegoNo ratings yet
- Anatomy & Physiology of The KidneyDocument27 pagesAnatomy & Physiology of The Kidneyraquel maniegoNo ratings yet
- Sci ConceptmapDocument1 pageSci Conceptmapraquel maniegoNo ratings yet
- Alteration in OxygenationDocument8 pagesAlteration in Oxygenationraquel maniegoNo ratings yet
- Stoma Care 01Document13 pagesStoma Care 01raquel maniegoNo ratings yet
- Concept Map NephrolithiasisDocument1 pageConcept Map Nephrolithiasisraquel maniegoNo ratings yet
- Components of FHSISDocument3 pagesComponents of FHSISraquel maniegoNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Gram Staining Protocol or ProcedureDocument4 pagesGram Staining Protocol or Procedurearavindbt2523No ratings yet
- Connective TissueDocument62 pagesConnective Tissuehnm mnhNo ratings yet
- Immunology Exam Q's With AnswersDocument26 pagesImmunology Exam Q's With AnswersHavardKrovel87% (55)
- PMDC NEB Exams Free Course BookletDocument8 pagesPMDC NEB Exams Free Course BookletDaxtren HicksNo ratings yet
- Menstrual Cycle PhasesDocument2 pagesMenstrual Cycle PhasesPatricia G ChiuNo ratings yet
- Dwnload Full Anatomy and Physiology 1st Edition Mckinley Solutions Manual PDFDocument35 pagesDwnload Full Anatomy and Physiology 1st Edition Mckinley Solutions Manual PDFleo7mco100% (17)
- Physical ExamDocument1 pagePhysical ExamJan DamesNo ratings yet
- Science ReviewerDocument13 pagesScience ReviewerLenie MatanguihanNo ratings yet
- Physical Characteristics of The NewbornDocument3 pagesPhysical Characteristics of The NewbornNica Mariz Dela CruzNo ratings yet
- ThyroidDocument7 pagesThyroidverawoNo ratings yet
- Rujukan OktoberDocument15 pagesRujukan Oktoberendang sunarmNo ratings yet
- Histologie Généralité Et Tissu Epithelume PDFDocument2 pagesHistologie Généralité Et Tissu Epithelume PDFشكوب ستانNo ratings yet
- (CLINPATH) 2.02 Transfusion II - Dr.-VillamayorDocument7 pages(CLINPATH) 2.02 Transfusion II - Dr.-VillamayorpasambalyrradjohndarNo ratings yet
- Respiratory Physiology: Control of The Upper Airway: Richard L. Horner University of TorontoDocument8 pagesRespiratory Physiology: Control of The Upper Airway: Richard L. Horner University of TorontoDopamina PsicoactivaNo ratings yet
- Snake AnatomyDocument7 pagesSnake AnatomyAdrin Ma'rufNo ratings yet
- Normocytic Normochromic AnemiaDocument18 pagesNormocytic Normochromic AnemiaElaizha PagulayanNo ratings yet
- List of Surgical ProceduresDocument3 pagesList of Surgical ProceduresAtto AmpereNo ratings yet
- Medico Legal CertificateDocument2 pagesMedico Legal CertificateJoanne besoyNo ratings yet
- Normal Delivery Checklist 2020Document4 pagesNormal Delivery Checklist 2020Ever Seneca EscaLeraNo ratings yet
- Nervous System - Anatomy & PhysiologyDocument2 pagesNervous System - Anatomy & PhysiologykathzheinNo ratings yet
- Grade 9 ScienceDocument19 pagesGrade 9 ScienceChristine Grace GiradoNo ratings yet
- June 2016 (v3) QP - Paper 2 CIE Biology IGCSEDocument20 pagesJune 2016 (v3) QP - Paper 2 CIE Biology IGCSEKamikazi GloriaNo ratings yet
- Digestive SystemDocument45 pagesDigestive SystemEzequiel ManluluNo ratings yet
- Embriologi Tumbuhan - Materi 2Document21 pagesEmbriologi Tumbuhan - Materi 2gahanNo ratings yet
- Mcqs in Medical Physiology For Pgmee Esp May 2010Document148 pagesMcqs in Medical Physiology For Pgmee Esp May 2010same20086% (21)
- Immunity and Vaccination RecordedDocument49 pagesImmunity and Vaccination RecordedMOMINAH AbbasiNo ratings yet
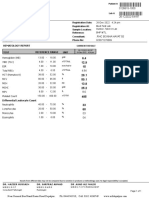
- BILAL FARID, 1 Year(s) /male: Registration Date: M.R. No: Registration At: Sample LocationDocument1 pageBILAL FARID, 1 Year(s) /male: Registration Date: M.R. No: Registration At: Sample LocationsaifNo ratings yet
- Liver Function TestsDocument28 pagesLiver Function TestsDr. Ashish Jawarkar100% (2)
- Skeletal System4Document1 pageSkeletal System4Elisha DienteNo ratings yet
- Exchange TransfusionDocument35 pagesExchange Transfusionsobinjohnpkl100% (2)