You might also like
- Website Planning Template ForDocument10 pagesWebsite Planning Template ForDeepak Veer100% (2)
- Nursing JudgementDocument6 pagesNursing Judgementapi-508142358No ratings yet
- Responding To Ten Common Delirium MisconceptionsDocument7 pagesResponding To Ten Common Delirium MisconceptionsFelipe Rangel Hassey100% (1)
- Situational Low Self-Esteem - NCPDocument3 pagesSituational Low Self-Esteem - NCPLizzey YuNo ratings yet
- Nursing Care Plan: Risk For Ineffective Airway Clearance Related To Bleeding From Tonsillectomy Short TermDocument4 pagesNursing Care Plan: Risk For Ineffective Airway Clearance Related To Bleeding From Tonsillectomy Short TermErika Danalle ArceoNo ratings yet
- Word SmartDocument189 pagesWord SmartSmeeta Prasai0% (1)
- NCP For PCAPDocument4 pagesNCP For PCAPDianeNo ratings yet
- Sunday: Monday Tuesday Wednesday Thursday Friday SaturdayDocument1 pageSunday: Monday Tuesday Wednesday Thursday Friday Saturdaybrucemartin3No ratings yet
- Filipinas Broadcasting Network Inc V Ago DigestDocument4 pagesFilipinas Broadcasting Network Inc V Ago DigestDYbieNo ratings yet
- Disenfranchised Grief and Physician BurnoutDocument4 pagesDisenfranchised Grief and Physician BurnoutAnthony VasconezNo ratings yet
- MRS. Erlinda M. Ko, RN, BSNDocument5 pagesMRS. Erlinda M. Ko, RN, BSNPrince MonNo ratings yet
- Disturbed Thought Process NCP Gallano May 22 2018Document3 pagesDisturbed Thought Process NCP Gallano May 22 2018Charles Mallari ValdezNo ratings yet
- Detailed Lesson Plan in Science VDocument6 pagesDetailed Lesson Plan in Science VMae LleovitNo ratings yet
- Level 6 Diploma in Business ManagementDocument4 pagesLevel 6 Diploma in Business ManagementGibsonNo ratings yet
- Affidavit of Consent To AdoptDocument2 pagesAffidavit of Consent To AdoptJohn Jeric LimNo ratings yet
- Breaking Bad News - ReflectionDocument6 pagesBreaking Bad News - ReflectionUZNAPM50% (2)
- 2 - EndometriosisDocument3 pages2 - EndometriosisJayson Olile100% (1)
- A Critical Review of Benedict AndersonDocument7 pagesA Critical Review of Benedict AndersonMatt Cromwell100% (10)
- Ease of Screening For Depression and DeliriumDocument6 pagesEase of Screening For Depression and DeliriumThaísa NogueiraNo ratings yet
- The Doctor-Patient RelationshipDocument9 pagesThe Doctor-Patient Relationshipravi dadlani parasramNo ratings yet
- Theoretical Foundation in NursingDocument15 pagesTheoretical Foundation in NursingLucia Paula OcileNo ratings yet
- Burnout, Compassion FatigueDocument8 pagesBurnout, Compassion Fatiguepatricio VelasquezNo ratings yet
- Patricia BennerDocument22 pagesPatricia BennerMatt MasilonganNo ratings yet
- The Unique Function of Nurse Case Managers On Psychiatric Units in Acute Care HospitalsDocument2 pagesThe Unique Function of Nurse Case Managers On Psychiatric Units in Acute Care Hospitalsacma2010No ratings yet
- DR-RLE-NCP-AND-DRUG-STUDY-Ambrosio 3Document6 pagesDR-RLE-NCP-AND-DRUG-STUDY-Ambrosio 3Ambrosio, Jasmin G.No ratings yet
- NCP IneffectiveHealthMaintenanceDM2Document3 pagesNCP IneffectiveHealthMaintenanceDM2Arone SebastianNo ratings yet
- Lorenzetti Et Al, 2013 PDFDocument7 pagesLorenzetti Et Al, 2013 PDFTANIAMSMNo ratings yet
- Risk OsteoDocument2 pagesRisk OsteoArone SebastianNo ratings yet
- A Medical Director's Perspective: A Case Study of Case EscalationDocument1 pageA Medical Director's Perspective: A Case Study of Case Escalationacma2010No ratings yet
- Heidi 467Document3 pagesHeidi 467Medicina UFU 92No ratings yet
- TFN - Patricia BennerDocument8 pagesTFN - Patricia BennerJelvi Maris LoyolaNo ratings yet
- NCPDMDocument2 pagesNCPDMArone SebastianNo ratings yet
- Managing Difficult Encounters. Understanding Physician, Patient, and Situational Factors (1) 1Document7 pagesManaging Difficult Encounters. Understanding Physician, Patient, and Situational Factors (1) 1Andrés PomboNo ratings yet
- Game Name LIFE THE GAME Stay SafeDocument9 pagesGame Name LIFE THE GAME Stay SafeJASTINE JOY PEREZNo ratings yet
- Canfamphys00078 0075Document4 pagesCanfamphys00078 0075Aseful Haque NafeeNo ratings yet
- Caring For Elderly Patients With Dementia Nursing PDFDocument11 pagesCaring For Elderly Patients With Dementia Nursing PDFAhmed MasoudNo ratings yet
- Caring For Elderly Patients With Dementia Nursing PDFDocument11 pagesCaring For Elderly Patients With Dementia Nursing PDFElla OrtizNo ratings yet
- NCP-and-Drug-study For MENDocument8 pagesNCP-and-Drug-study For MENVillie SumandeNo ratings yet
- Faye Abdellah HandoutDocument4 pagesFaye Abdellah HandoutMyra Flores100% (2)
- Nursing Care Plan: Risk For Ineffective Airway Clearance Related To Bleeding From Tonsillectomy Short TermDocument4 pagesNursing Care Plan: Risk For Ineffective Airway Clearance Related To Bleeding From Tonsillectomy Short TermErika Danalle ArceoNo ratings yet
- Responding To Ten Common Delirium Misconceptions With Best Evidence: An Educational Review For CliniciansDocument7 pagesResponding To Ten Common Delirium Misconceptions With Best Evidence: An Educational Review For CliniciansdkdkdsNo ratings yet
- 3 Nursing Care PlanDocument6 pages3 Nursing Care PlanJeyser T. GamutiaNo ratings yet
- Nursing Care Plan: Risk For Ineffective Airway Clearance Related To Bleeding From Tonsillectomy Short TermDocument4 pagesNursing Care Plan: Risk For Ineffective Airway Clearance Related To Bleeding From Tonsillectomy Short TermErika Danalle ArceoNo ratings yet
- A Case Study Application of Orem's Care Deficit Theory and Standardized Nursing Languages in A Case Study in A Women With DiabetesDocument3 pagesA Case Study Application of Orem's Care Deficit Theory and Standardized Nursing Languages in A Case Study in A Women With DiabetesLady Jane CaguladaNo ratings yet
- JMH 2004 000164Document8 pagesJMH 2004 000164MrEnttNo ratings yet
- Everyday Ethics in An Acute Psychiatric UnitDocument4 pagesEveryday Ethics in An Acute Psychiatric Unitsetya indahNo ratings yet
- Hypoactive Delirium: Christian Hosker, David WardDocument5 pagesHypoactive Delirium: Christian Hosker, David Wardjohnny chawNo ratings yet
- 203 Module 2 - NCP - GestaDocument3 pages203 Module 2 - NCP - Gestahaxa yzaNo ratings yet
- Transcultural-Nursing-Notes-Ppt-Only 1Document2 pagesTranscultural-Nursing-Notes-Ppt-Only 1Genierose YantoNo ratings yet
- Cues/Data Nursing Diagnosis Interference Planning Intervention Rationale EvaluationDocument3 pagesCues/Data Nursing Diagnosis Interference Planning Intervention Rationale EvaluationLouwella RamosNo ratings yet
- Ethics of Nursing Shift ReportDocument5 pagesEthics of Nursing Shift ReportkelllyNo ratings yet
- Delirium: Section I: Scenario DemographicsDocument6 pagesDelirium: Section I: Scenario DemographicsNikey LimNo ratings yet
- Ethical and Legal Considerations: Type of Problem ExampleDocument8 pagesEthical and Legal Considerations: Type of Problem ExampleAce Khiel PeraltaNo ratings yet
- Con Ict Management, Prevention, and Resolution in Medical SettingsDocument6 pagesCon Ict Management, Prevention, and Resolution in Medical SettingsRio Handi SanjayaNo ratings yet
- Ban - Final Evidence Case Analysis PortfolioDocument2 pagesBan - Final Evidence Case Analysis PortfolioDanielle Audrey BanNo ratings yet
- Nursing Care Plan For Premature Rupture of MembranesDocument2 pagesNursing Care Plan For Premature Rupture of MembranesGEN COLLANTESNo ratings yet
- Managing Difficult Patient Encounters (AAFP 2023)Document7 pagesManaging Difficult Patient Encounters (AAFP 2023)Breno Resende Rodrigues CunhaNo ratings yet
- The Patient%u2019s Experience With Critical IllnessDocument15 pagesThe Patient%u2019s Experience With Critical IllnessineNo ratings yet
- PIIS0008418219312797-2 - Xochitl Duque AlarconDocument10 pagesPIIS0008418219312797-2 - Xochitl Duque AlarconOscar GarzaNo ratings yet
- Midterm 3021Document9 pagesMidterm 3021api-283170120No ratings yet
- Eugenio Preeclampsia NCPDocument2 pagesEugenio Preeclampsia NCPBethrice MelegritoNo ratings yet
- The Practice of Medical Referral: Ethical ConcernsDocument5 pagesThe Practice of Medical Referral: Ethical ConcernsGarry SoloanNo ratings yet
- Moleno NCPDocument11 pagesMoleno NCPMissy U. TorrechillaNo ratings yet
- MindfulnessDocument2 pagesMindfulnessAndreaBuitragoMalaverNo ratings yet
- Design and The Bottom Line:: Practical Patient-Centered Approaches To The Physical EnvironmentDocument21 pagesDesign and The Bottom Line:: Practical Patient-Centered Approaches To The Physical EnvironmentindahNo ratings yet
- Thij 18 6842Document5 pagesThij 18 6842Zahira Mari GuillenNo ratings yet
- Am J Crit Care-2015-Rushton-412-20 PDFDocument11 pagesAm J Crit Care-2015-Rushton-412-20 PDFOwais ZiaNo ratings yet
- Developing A Palliative Care Service: One Hospital's ExperienceDocument2 pagesDeveloping A Palliative Care Service: One Hospital's Experienceacma2010No ratings yet
- Getting The Most From Consultant Resources: by Martha J. Koen, ACM, MN, RNDocument2 pagesGetting The Most From Consultant Resources: by Martha J. Koen, ACM, MN, RNacma2010No ratings yet
- Extending Care Beyond Hospital Walls: Follow-Up Program Impacts Patients and Addresses Post-Discharge NeedsDocument3 pagesExtending Care Beyond Hospital Walls: Follow-Up Program Impacts Patients and Addresses Post-Discharge Needsacma2010No ratings yet
- My Magnificent Seven' - How Case Management Assistants Turbo-Charge The Case Management FunctionDocument2 pagesMy Magnificent Seven' - How Case Management Assistants Turbo-Charge The Case Management Functionacma2010No ratings yet
- A Medical Director's PerspectiveDocument4 pagesA Medical Director's Perspectiveacma2010No ratings yet
- 2010 V 8 I 3 A 3Document3 pages2010 V 8 I 3 A 3acma2010No ratings yet
- Opening The Door To Timely and Informative DischargeDocument3 pagesOpening The Door To Timely and Informative Dischargeacma2010No ratings yet
- Oncology Case Management Across The Continuum of Care: by Amelia Williams, MSWDocument2 pagesOncology Case Management Across The Continuum of Care: by Amelia Williams, MSWacma2010No ratings yet
- A Management Engineering Approach To Improving Throughput and Shortening Overall LOS: An Unique Model For Efficiency and Time StudyDocument2 pagesA Management Engineering Approach To Improving Throughput and Shortening Overall LOS: An Unique Model For Efficiency and Time Studyacma2010No ratings yet
- Capturing Return On Investment For Case Management Services: by Vickie Alexander Knight, RN, BS, CCMDocument3 pagesCapturing Return On Investment For Case Management Services: by Vickie Alexander Knight, RN, BS, CCMacma2010No ratings yet
- The Critical Role of Clinical Social Work in Case ManagementDocument2 pagesThe Critical Role of Clinical Social Work in Case Managementacma2010No ratings yet
- Discharge Screening: Emergency Department Case Managers Help Improve Compliance With Discharge InstructionsDocument3 pagesDischarge Screening: Emergency Department Case Managers Help Improve Compliance With Discharge Instructionsacma2010No ratings yet
- Discharge Screening: Emergency Department Case Managers Help Improve Compliance With Discharge InstructionsDocument2 pagesDischarge Screening: Emergency Department Case Managers Help Improve Compliance With Discharge Instructionsacma2010No ratings yet
- Case Manager Certification Offers Unique Practice-Specific ValidationDocument2 pagesCase Manager Certification Offers Unique Practice-Specific Validationacma2010No ratings yet
- Emergency Department Gatekeepers - Interventions With Chronic Pain Patients and Identity FraudDocument3 pagesEmergency Department Gatekeepers - Interventions With Chronic Pain Patients and Identity Fraudacma2010No ratings yet
- Issues in Pediatric Case Management: by Rhonda Cofield, MSW, LCSWDocument2 pagesIssues in Pediatric Case Management: by Rhonda Cofield, MSW, LCSWacma2010No ratings yet
- A View From The Field: Career Advancement Through Clinical LaddersDocument2 pagesA View From The Field: Career Advancement Through Clinical Laddersacma2010No ratings yet
- Supervision in Case Management: A Focus On Professional DevelopmentDocument3 pagesSupervision in Case Management: A Focus On Professional Developmentacma2010No ratings yet
- "Life Changes in The Instant. The Ordinary Instant ": Dying Well: Case Management Leads A Process Redesign ProjectDocument3 pages"Life Changes in The Instant. The Ordinary Instant ": Dying Well: Case Management Leads A Process Redesign Projectacma2010No ratings yet
- A Medical Director's PerspectiveDocument2 pagesA Medical Director's Perspectiveacma2010No ratings yet
- A View From The Field: Emergency Department Case Managers Support Innovation That Improves Hospital RevenueDocument2 pagesA View From The Field: Emergency Department Case Managers Support Innovation That Improves Hospital Revenueacma2010No ratings yet
- Organization and Its EnvironmentDocument20 pagesOrganization and Its EnvironmentPrasanga PriyankaranNo ratings yet
- Class Mural ProjectDocument1 pageClass Mural ProjectarianamoonNo ratings yet
- IBPS RRB Office Assistant Exam Pattern: Get Free Job Alerts in Your Email Click HereDocument9 pagesIBPS RRB Office Assistant Exam Pattern: Get Free Job Alerts in Your Email Click Hereहिमाँशु गंगवानीNo ratings yet
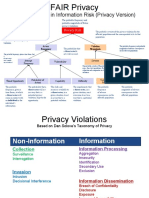
- Factor Analysis in Information Risk (Privacy Version)Document8 pagesFactor Analysis in Information Risk (Privacy Version)Otgonbayar TsengelNo ratings yet
- Ielts WritingDocument18 pagesIelts Writinghai_jim0% (1)
- Curriculum Map Physical Education 6-8Document7 pagesCurriculum Map Physical Education 6-8Levine Del ValleNo ratings yet
- Car Modification and Accessories Business Plan Executive SummaryDocument9 pagesCar Modification and Accessories Business Plan Executive Summaryjunaidjavaid99No ratings yet
- Ceferino Paredes, Jr. Vs SandiganbayanDocument4 pagesCeferino Paredes, Jr. Vs SandiganbayanRoseanne MateoNo ratings yet
- Sleeping PodsDocument1 pageSleeping PodsSamrin ZeyaNo ratings yet
- PPIC Training ResumeDocument2 pagesPPIC Training Resumenana arya sumardjaNo ratings yet
- ACORD v. ZamoraDocument31 pagesACORD v. ZamoraPrincess Samantha SarcedaNo ratings yet
- It's All About That DANCE: The D AnceDocument3 pagesIt's All About That DANCE: The D AnceRyzza Yvonne MedalleNo ratings yet
- Akbar, Emperor of India by Garbe, Richard Von, 1857-1927Document31 pagesAkbar, Emperor of India by Garbe, Richard Von, 1857-1927Gutenberg.orgNo ratings yet
- Chapter 12 Quiz 1Document4 pagesChapter 12 Quiz 1joyceNo ratings yet
- Eapp Quarter 2 Module 3 (Jenny Mae D. Otto Grade 12 Abm-Yen)Document12 pagesEapp Quarter 2 Module 3 (Jenny Mae D. Otto Grade 12 Abm-Yen)Jenny Mae OttoNo ratings yet
- A B Keith (Ed) - Speeches and Documents On Indian Policy 1750-1921 Vol IIDocument394 pagesA B Keith (Ed) - Speeches and Documents On Indian Policy 1750-1921 Vol IIfahmed3010No ratings yet
- 4IR Framework Presentation - FINALDocument56 pages4IR Framework Presentation - FINALNathanNo ratings yet
- Animals and Human Language (Unit 02)Document2 pagesAnimals and Human Language (Unit 02)Maryam Raza100% (1)
- RADIO COMMUNICATIONS OF THE PHILIPPINES, INC. (RCPI), Petitioner, Vs - ALFONSO VERCHEZDocument4 pagesRADIO COMMUNICATIONS OF THE PHILIPPINES, INC. (RCPI), Petitioner, Vs - ALFONSO VERCHEZVenus Jane FinuliarNo ratings yet
- Manipur Public Service Commission SyllabusDocument9 pagesManipur Public Service Commission SyllabusJohn LoukrakpamNo ratings yet
- Muhammad Alif B. Mohd AnuarDocument2 pagesMuhammad Alif B. Mohd AnuarAlif AnuarNo ratings yet