You might also like
- Pre Fitness Form - 13.09.2021Document2 pagesPre Fitness Form - 13.09.2021JindalNo ratings yet
- Fitness Form 08.09.2020Document4 pagesFitness Form 08.09.2020Yogesh PatelNo ratings yet
- Pre Fitness FormDocument2 pagesPre Fitness FormNihasNo ratings yet
- Registration FormDocument3 pagesRegistration Formsimon farrellNo ratings yet
- Health CertificateDocument2 pagesHealth CertificateChristos YiangouNo ratings yet
- Chest Pain Questionnaire - Applicant 2020Document3 pagesChest Pain Questionnaire - Applicant 2020Via B. BorrezNo ratings yet
- Physician's Examination: Health FormDocument1 pagePhysician's Examination: Health FormOswald ErazoNo ratings yet
- Health Action PlanDocument20 pagesHealth Action PlanCielito GumbanNo ratings yet
- Npdmdu Medical Evaluation Form 2023Document2 pagesNpdmdu Medical Evaluation Form 2023Substationsix MalaboncpsNo ratings yet
- Medical Examintation Report: Document No MTIPL/HR/F0006 1Document1 pageMedical Examintation Report: Document No MTIPL/HR/F0006 1Kabir ShelkeNo ratings yet
- Pre Medical Evaluatiom Form PFT 1 PDFDocument2 pagesPre Medical Evaluatiom Form PFT 1 PDFAIEN WENDELEIH Q. CAPINPIN100% (1)
- Physical Activity Readiness Questionnaire (PAR-Q)Document2 pagesPhysical Activity Readiness Questionnaire (PAR-Q)eternalkainNo ratings yet
- 3 Health PDFDocument2 pages3 Health PDFAndré DomanskiNo ratings yet
- Health Questionnaire TemplateDocument2 pagesHealth Questionnaire TemplateBaxwal AxmedNo ratings yet
- 3 Health PDFDocument2 pages3 Health PDFpierlisurNo ratings yet
- MFC PDFDocument5 pagesMFC PDFdipmipNo ratings yet
- Physical Examination Report: 23/FEMALE Dalig, Balayan, Batangas 7/11/1997 8:50 AM Waltermart Balayan 6/4/2021 SingleDocument3 pagesPhysical Examination Report: 23/FEMALE Dalig, Balayan, Batangas 7/11/1997 8:50 AM Waltermart Balayan 6/4/2021 SingleIan De LeonNo ratings yet
- Medical Evaluation Form 2022Document2 pagesMedical Evaluation Form 2022jimmy p. lamhi50% (2)
- 57035d7950aaf-BCCI TUE Application Form V1.2015 PDFDocument3 pages57035d7950aaf-BCCI TUE Application Form V1.2015 PDFbhavyapruthiNo ratings yet
- OGUK Medical FormDocument7 pagesOGUK Medical Formum erNo ratings yet
- Pilates Private Session Policies and ProceduresDocument7 pagesPilates Private Session Policies and ProceduresEric LeeNo ratings yet
- Practice Full Manual-1-12Document12 pagesPractice Full Manual-1-12p7hgzmkct4No ratings yet
- Envelope - Medical Application Form - New - V3 - Mednet - 1Document3 pagesEnvelope - Medical Application Form - New - V3 - Mednet - 1muhdm7771No ratings yet
- Health Questionnaire CandidateDocument5 pagesHealth Questionnaire CandidateSaudia Arabia JobsNo ratings yet
- Medical Application Form: Insured Name: Inception DateDocument3 pagesMedical Application Form: Insured Name: Inception DateDidier G PeñuelaNo ratings yet
- Medical Application Form: Name Relation (E/S/C) D. O. B SEX (M/F) Marital Status Height (CM) Weight (KG) Emirates (VISA)Document3 pagesMedical Application Form: Name Relation (E/S/C) D. O. B SEX (M/F) Marital Status Height (CM) Weight (KG) Emirates (VISA)cmthebossNo ratings yet
- Parq EditedDocument2 pagesParq EditedJay Ann AgarradoNo ratings yet
- KTS - Medical History Questionnaire by DRDocument6 pagesKTS - Medical History Questionnaire by DRtaufikmat442No ratings yet
- Form Pemfis Dokter (Subcon Saipem)Document3 pagesForm Pemfis Dokter (Subcon Saipem)Humas PemasaranNo ratings yet
- Health Certificate PDFDocument2 pagesHealth Certificate PDFPedro KunstNo ratings yet
- Medical NarrativeDocument3 pagesMedical NarrativeJennessee MiagueNo ratings yet
- Par QDocument2 pagesPar Qaicel sagaNo ratings yet
- DischargesummaryDocument2 pagesDischargesummaryepi bahoNo ratings yet
- Diabetes+mellitus+questionnaire ApplicantDocument2 pagesDiabetes+mellitus+questionnaire ApplicantClaudine Limasa TabudlongNo ratings yet
- Personal Sheet (Stammdatenblatt)Document2 pagesPersonal Sheet (Stammdatenblatt)kocis075No ratings yet
- Himalayas 2022: Medical FormDocument4 pagesHimalayas 2022: Medical FormDeepak WaradNo ratings yet
- AXA Hypertension QuestionnaireDocument2 pagesAXA Hypertension QuestionnaireClaudine Limasa TabudlongNo ratings yet
- Medical Form & Document ChecklistDocument2 pagesMedical Form & Document Checklistrjadhav0075No ratings yet
- Year 9 Camp Health and Medical ConsentDocument3 pagesYear 9 Camp Health and Medical ConsentFiona CharringtonNo ratings yet
- Format Pre EmploymentDocument10 pagesFormat Pre EmploymentNurman HidayatNo ratings yet
- Prashant Kumar-2Document3 pagesPrashant Kumar-2prashantp7819980No ratings yet
- Medical CertificateDocument1 pageMedical CertificateSupriyo GhoshNo ratings yet
- Student Medical RecordDocument3 pagesStudent Medical Recordhamsa RasbiehNo ratings yet
- RCL Employment Medical Examination Form A (New-Returning) Revised 2015-03Document2 pagesRCL Employment Medical Examination Form A (New-Returning) Revised 2015-03Ahmad ShodiqNo ratings yet
- Medical Form - GafDocument1 pageMedical Form - GafHenry AmoakoNo ratings yet
- (A Questionnaire For People Aged 15 To 69) : YES To One or More QuestionsDocument3 pages(A Questionnaire For People Aged 15 To 69) : YES To One or More QuestionsTeraza, JeannieNo ratings yet
- JTL FM HR 004 Medical QuestionnaireDocument3 pagesJTL FM HR 004 Medical QuestionnairepeterNo ratings yet
- Pharmacist Workup of Drug Therapy in Pharmaceutical Care: Problem Oriented Pharmacist RecordDocument22 pagesPharmacist Workup of Drug Therapy in Pharmaceutical Care: Problem Oriented Pharmacist RecordputihatauhitamNo ratings yet
- Attachment 5 - Crew Health Declaration - 2015-09 - Ver0 (5) 2Document1 pageAttachment 5 - Crew Health Declaration - 2015-09 - Ver0 (5) 2Julessio SihombingNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormUzair KhalidNo ratings yet
- My Family's Health RecordDocument2 pagesMy Family's Health RecordQurat-ul-Ain AzamNo ratings yet
- Claims Aps Hi MR SurgicalDocument3 pagesClaims Aps Hi MR SurgicalRudolf CunananNo ratings yet
- UHS Pre-Enrolment Med Clearance - FinalDocument3 pagesUHS Pre-Enrolment Med Clearance - FinalMikayla DutingNo ratings yet
- Online QuestionnaireDocument17 pagesOnline QuestionnaireAJAY RAJBHARNo ratings yet
- Health Assessment Questionnaire-English R1Document4 pagesHealth Assessment Questionnaire-English R1JakariaNo ratings yet
- Application For Healthcheckup PDFDocument5 pagesApplication For Healthcheckup PDFNishant ChowhanNo ratings yet
- Application and Health PDFDocument2 pagesApplication and Health PDFMunawwar MuhammedNo ratings yet
- Health DeclarationDocument5 pagesHealth Declarationust dol100% (1)
- Dnacprform AdultDocument1 pageDnacprform Adultlegend789No ratings yet
- Cough - AMBOSSDocument12 pagesCough - AMBOSSAmira AlmutairiNo ratings yet
- 22q11.2 GPC 2023Document24 pages22q11.2 GPC 2023Antoine NinoNo ratings yet
- Circulatory System ActivityDocument7 pagesCirculatory System ActivityReginald MalibiranNo ratings yet
- Primer: Acute Kidney InjuryDocument17 pagesPrimer: Acute Kidney InjuryDiana AngelesNo ratings yet
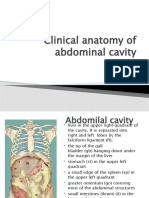
- Clinical Anatomy of Abdominal CavityDocument88 pagesClinical Anatomy of Abdominal CavityFahim NadvyNo ratings yet
- Frog Dissection GizmoDocument6 pagesFrog Dissection GizmoNithya MajetiNo ratings yet
- Peran Perawat Dalam Penangan Kegawatn Jantung - ERWIN (Autosaved)Document64 pagesPeran Perawat Dalam Penangan Kegawatn Jantung - ERWIN (Autosaved)Adrianus AdrianusNo ratings yet
- Digestive SystemDocument2 pagesDigestive SystemRashid DayaoNo ratings yet
- MPMSU MBBS 1st Year Previous Year Questions (2015-2023)Document83 pagesMPMSU MBBS 1st Year Previous Year Questions (2015-2023)Koshtubh Pratap Singh PariharNo ratings yet
- Paper OSADocument21 pagesPaper OSAEliska YantiNo ratings yet
- E.C.G Machine: by Er.U.Karthik Premkumar, H.O.D - Biomedical Engineering DepartmentDocument36 pagesE.C.G Machine: by Er.U.Karthik Premkumar, H.O.D - Biomedical Engineering DepartmentAch ThungNo ratings yet
- 058+ +1595+ +Luh+Made+Indrasuari+ +galleyDocument5 pages058+ +1595+ +Luh+Made+Indrasuari+ +galleyLathief CaakNo ratings yet
- 2012 Medtronic Coronary CatalogDocument114 pages2012 Medtronic Coronary Catalogmihalcea alin0% (1)
- Interventions of Postpartum Hemorrhage.16Document17 pagesInterventions of Postpartum Hemorrhage.16Fernando Peralta PalmezanoNo ratings yet
- Cardiology 2023 FinalDocument208 pagesCardiology 2023 FinalBelinda ELISHA100% (1)
- Which Is More Accurate in Measuring The Blood Pressure? A Digital or An Aneroid SphygmomanometerDocument4 pagesWhich Is More Accurate in Measuring The Blood Pressure? A Digital or An Aneroid SphygmomanometerSri YatiNo ratings yet
- TMS ChecklistDocument1 pageTMS ChecklistMuhammad HussnainNo ratings yet
- Path Pancreas McqsDocument4 pagesPath Pancreas McqsUu UuNo ratings yet
- 3 MAJOR OPENINGS /right Atirum: Cardiovascular System Serious PericardiumDocument3 pages3 MAJOR OPENINGS /right Atirum: Cardiovascular System Serious PericardiumAebee Alcaraz100% (1)
- Juno Tech Sheet-Flyer v5Document2 pagesJuno Tech Sheet-Flyer v5Divina BlancoNo ratings yet
- Modern Nursing Cardiogenic Pulmonary Edema Seminar HARKIT SugiyonoDocument43 pagesModern Nursing Cardiogenic Pulmonary Edema Seminar HARKIT SugiyonoeffitaNo ratings yet
- Citicoline Drug StudyDocument2 pagesCiticoline Drug StudyJC LumayaNo ratings yet
- Dwnload Full Little and Falaces Dental Management of The Medically Compromised Patient 8th Edition Little Test Bank PDFDocument36 pagesDwnload Full Little and Falaces Dental Management of The Medically Compromised Patient 8th Edition Little Test Bank PDFdanagarzad90y100% (10)
- 2019 - ESC - Guidelines SLIDESDocument23 pages2019 - ESC - Guidelines SLIDESFa CurieNo ratings yet
- European Journal of Internal MedicineDocument4 pagesEuropean Journal of Internal Medicinesamer battatNo ratings yet
- Assessment of HypertensionDocument44 pagesAssessment of HypertensionGrow HealthyNo ratings yet
- Cardiologia Croatica 2021 16 - 1-2 - 83Document1 pageCardiologia Croatica 2021 16 - 1-2 - 83daia4322746No ratings yet
- Aula 1 - Tracheobronchial BranchingDocument16 pagesAula 1 - Tracheobronchial BranchingThiago StoianovNo ratings yet
- PDA Case StudyDocument5 pagesPDA Case StudyDiana Andrea AyongaoNo ratings yet
- BPJ Vol 14 No 2 P 961-969Document9 pagesBPJ Vol 14 No 2 P 961-969Sifa ShopingNo ratings yet