You might also like
- Atelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesFrom EverandAtelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesNo ratings yet
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Bronchospasm PR 1Document41 pagesBronchospasm PR 1teklayNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- HW InotropesDocument3 pagesHW InotropesNatalie YeohNo ratings yet
- Practice Standards For The Emergency Nurse Specialist. CENA, 2014Document16 pagesPractice Standards For The Emergency Nurse Specialist. CENA, 2014Cristobal Alejandro Falado SantanderNo ratings yet
- ACLS Algorithms Adult 2010 Revised May 31 2011Document12 pagesACLS Algorithms Adult 2010 Revised May 31 2011arturschander3614No ratings yet
- Vascular Responses to PathogensFrom EverandVascular Responses to PathogensFelicity N.E. GavinsNo ratings yet
- Chest Trauma FinalDocument50 pagesChest Trauma FinalAsim Siddiq VineNo ratings yet
- Acls Course HandoutsDocument8 pagesAcls Course HandoutsRoxas CedrickNo ratings yet
- Mechanical Ventilation and Intracranial PressureDocument30 pagesMechanical Ventilation and Intracranial PressureFlavius AnghelNo ratings yet
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNo ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Lung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesFrom EverandLung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesAlain JunodNo ratings yet
- Inotropes, Excellent Article, With DosingDocument47 pagesInotropes, Excellent Article, With DosingNavojit ChowdhuryNo ratings yet
- Leading U: Inspirational Stories from UAlberta Alumni & StudentsFrom EverandLeading U: Inspirational Stories from UAlberta Alumni & StudentsNo ratings yet
- Chronic BronchitisDocument2 pagesChronic BronchitisEimhie Lee CasiNo ratings yet
- Swan Ganz CathetersDocument27 pagesSwan Ganz CatheterschadchimaNo ratings yet
- Suctioning Artificial Airways - AdultsDocument27 pagesSuctioning Artificial Airways - AdultssdaNo ratings yet
- Abnormal Slow Heart Beats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAbnormal Slow Heart Beats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Cardiac II Study GuideDocument6 pagesCardiac II Study GuiderunnermnNo ratings yet
- Lung Transplant PathwayDocument39 pagesLung Transplant PathwayMohana Preethi MNo ratings yet
- Care of Patient With TPM Slide PresentationDocument16 pagesCare of Patient With TPM Slide PresentationirzehronNo ratings yet
- Diabetic Ketoacidosis and Hyperosmolar Hyperglycaemic StateDocument55 pagesDiabetic Ketoacidosis and Hyperosmolar Hyperglycaemic StateEva PrimanandaNo ratings yet
- Drugs in Cardiac EnmergenciesDocument94 pagesDrugs in Cardiac EnmergenciesVijayan VelayudhanNo ratings yet
- Nervous System AlterationsDocument45 pagesNervous System AlterationsMajesty ParkerNo ratings yet
- Shock Types 141009102815 Conversion Gate01Document41 pagesShock Types 141009102815 Conversion Gate01Samjaisheel SamsonNo ratings yet
- A Nurse's Guide to Caring for Cardiac Intervention PatientsFrom EverandA Nurse's Guide to Caring for Cardiac Intervention PatientsNo ratings yet
- Thoracic Trauma: Kenyatta University LectureDocument25 pagesThoracic Trauma: Kenyatta University LectureIrene Zae MwandotoNo ratings yet
- ECG Dysrhthmias IIIDocument31 pagesECG Dysrhthmias IIIAmani KayedNo ratings yet
- Medical Surgical Nursing Critical Thinking in Patient Care Single Volume 4th Edition Lemone Test BankDocument4 pagesMedical Surgical Nursing Critical Thinking in Patient Care Single Volume 4th Edition Lemone Test BankRebeccaGilliamNo ratings yet
- Arterial LinesDocument9 pagesArterial LinesRei IrincoNo ratings yet
- MVR CabgDocument57 pagesMVR CabgRoshani sharmaNo ratings yet
- CardioDocument7 pagesCardioGerald AndrinNo ratings yet
- Valvular Heart Disease 2Document46 pagesValvular Heart Disease 2Topea BogdanNo ratings yet
- Chest TubesDocument12 pagesChest TubesMark Hammerschmidt100% (4)
- Drugs in ObstetricsDocument95 pagesDrugs in ObstetricsPriya jNo ratings yet
- Cad ....Document94 pagesCad ....AnanthibalaNo ratings yet
- CCU Clinical GuidelinesDocument63 pagesCCU Clinical GuidelinesHAMMYER ALROKHAMINo ratings yet
- Complications of Acute Myocardial InfarctionDocument5 pagesComplications of Acute Myocardial Infarctionlourdesfercab_at_msn100% (1)
- Cardiac CatheterizationDocument2 pagesCardiac Catheterizationjacallis50% (2)
- Critical Care SedationFrom EverandCritical Care SedationAngelo Raffaele De GaudioNo ratings yet
- Drug Dosage and IV Rates CalculationsDocument6 pagesDrug Dosage and IV Rates CalculationsLorens Troy SoltisNo ratings yet
- Arterial Lines in PACU: Presented by Autum Jacobs RN, BSNDocument34 pagesArterial Lines in PACU: Presented by Autum Jacobs RN, BSNinuko1212No ratings yet
- Asthma and CopdDocument44 pagesAsthma and CopdBeer Dilacshe100% (1)
- Pleural Fluid AnalysisDocument15 pagesPleural Fluid AnalysisNatalie Sarah MoonNo ratings yet
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Cardiovascular Disorders: BY: Maximin A. Pomperada, RN, MANDocument65 pagesCardiovascular Disorders: BY: Maximin A. Pomperada, RN, MANRellie Castro100% (1)
- Electrocardiogramm - Ecg InterpretationDocument56 pagesElectrocardiogramm - Ecg InterpretationKreshnik HAJDARI100% (1)
- 2012 AWMA Pan Pacific Guidelines PDFDocument124 pages2012 AWMA Pan Pacific Guidelines PDFhidayat0781No ratings yet
- Handouts - PsychiatricDocument4 pagesHandouts - Psychiatricsendang JNo ratings yet
- Dilatation and Curettage ProcedureDocument3 pagesDilatation and Curettage Proceduresagi muNo ratings yet
- Internship Report Noor Arshad 28Document80 pagesInternship Report Noor Arshad 28hammadNo ratings yet
- Attention Deficit-Hyperactive DisorderDocument3 pagesAttention Deficit-Hyperactive Disorderadan oladiveNo ratings yet
- Pulmonary Artery CatheterDocument32 pagesPulmonary Artery Catheterwaqas_xs100% (1)
- Types of WoundsDocument4 pagesTypes of WoundsHanarisha Putri AzkiaNo ratings yet
- Renal Function TestsDocument23 pagesRenal Function TestsKer YehunNo ratings yet
- Guidelines On Blood Cultures: Journal of Microbiology, Immunology and InfectionDocument3 pagesGuidelines On Blood Cultures: Journal of Microbiology, Immunology and InfectionSumesh Shreekhanda ShresthaNo ratings yet
- Introduction-: Article: Cobra Pose (Bhujangasana)Document3 pagesIntroduction-: Article: Cobra Pose (Bhujangasana)Saiteja Varma DatlaNo ratings yet
- JIA - Information For TeachersDocument4 pagesJIA - Information For TeachersragingreaderNo ratings yet
- Head InjuryDocument55 pagesHead InjuryDakaNo ratings yet
- Urinary Tract Infection (UTI) : Pharmacotherapeutics II YrDocument20 pagesUrinary Tract Infection (UTI) : Pharmacotherapeutics II YrpawannnnNo ratings yet
- Hand Hygiene Handout PDFDocument32 pagesHand Hygiene Handout PDFms RN100% (1)
- AppendectomyDocument8 pagesAppendectomyDark AghanimNo ratings yet
- Health Questionnaire TemplateDocument2 pagesHealth Questionnaire TemplateBaxwal AxmedNo ratings yet
- Daily Inspiration: Powered by Crystallive™Document8 pagesDaily Inspiration: Powered by Crystallive™douglaszimbaNo ratings yet
- GR2 Plasmodium-Spp PDFDocument29 pagesGR2 Plasmodium-Spp PDFEran Mark RojasNo ratings yet
- Ectopic Pregnancy: DR .Urmila KarkiDocument27 pagesEctopic Pregnancy: DR .Urmila KarkiBasudev chNo ratings yet
- Ciwa Ar PDFDocument2 pagesCiwa Ar PDFconheoconNo ratings yet
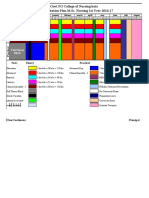
- 10.master Rotation Plan M. Sc. Nursing 1st YearDocument4 pages10.master Rotation Plan M. Sc. Nursing 1st YearNaresh JeengarNo ratings yet
- Obat Katalog Tahun 2017Document96 pagesObat Katalog Tahun 2017Aqim Apa AdanyaNo ratings yet
- Oral Contributions: JACC March 9, 2010 ABSTRACTS: Cardiac Arrhythmias A1Document217 pagesOral Contributions: JACC March 9, 2010 ABSTRACTS: Cardiac Arrhythmias A1Apner Calvin SuNo ratings yet
- Cardiac Glycosides 815Document19 pagesCardiac Glycosides 815SanskritiNo ratings yet
- NipedipinDocument4 pagesNipedipindesty sanzNo ratings yet
- Cleft Lip and Cleft PalateDocument16 pagesCleft Lip and Cleft PalateDeepthi ViswaroopanNo ratings yet
- 2010 Orthopaedic JournalDocument80 pages2010 Orthopaedic JournalPooria1989No ratings yet
- 9c5ff54e-92aa-4393-8350-218e91c128d2Document6 pages9c5ff54e-92aa-4393-8350-218e91c128d2Zarbakht AliNo ratings yet
- Benefits of The Costoclavicular Space For.15Document2 pagesBenefits of The Costoclavicular Space For.15andrew herringNo ratings yet
- Surgery Surgical Nursing Objs With AnsDocument136 pagesSurgery Surgical Nursing Objs With AnsmintahmeshackbenjaminNo ratings yet