You might also like
- Samir Rafla - Sudden Cardiac Death in Structurally Normal Hearts, Diagnosis and PreventionDocument55 pagesSamir Rafla - Sudden Cardiac Death in Structurally Normal Hearts, Diagnosis and Preventionsamir raflaNo ratings yet
- Treatment of Diabetes Mellitus T2 - Samir RaflaDocument35 pagesTreatment of Diabetes Mellitus T2 - Samir Raflasamir raflaNo ratings yet
- J Clin Exp Card-The Effect of Long Term Smoking As An Independent Coronary Risk Factor On Myocardial PerfusionDocument5 pagesJ Clin Exp Card-The Effect of Long Term Smoking As An Independent Coronary Risk Factor On Myocardial Perfusionsamir raflaNo ratings yet
- ICRJ-Validation of Cornell Product As A Method of Assessing Left Ventricular HypertrophyDocument5 pagesICRJ-Validation of Cornell Product As A Method of Assessing Left Ventricular Hypertrophysamir raflaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Nursing Process in Psychiatric NursingDocument9 pagesNursing Process in Psychiatric NursingIntellibrainNo ratings yet
- DC2020-0067 ICD-10 Code For COVID-19 (Previously Known As 2019-nCoV) (02-12-20)Document1 pageDC2020-0067 ICD-10 Code For COVID-19 (Previously Known As 2019-nCoV) (02-12-20)Leah Rose Figueroa ParasNo ratings yet
- TMS Chez Les InfimiersDocument38 pagesTMS Chez Les InfimierszouhireamNo ratings yet
- MeningokelDocument9 pagesMeningokelAisyah CahNo ratings yet
- F.A. 5 Health AssessmentDocument6 pagesF.A. 5 Health AssessmentYep YepNo ratings yet
- DR Pouyiouros-English PDFDocument2 pagesDR Pouyiouros-English PDFPantelis AshikkisNo ratings yet
- 2022 Year 10 Camp EXTREMEDocument11 pages2022 Year 10 Camp EXTREMEJohn BroughtonNo ratings yet
- ACTIVITY NO - 2 - MycologyDocument17 pagesACTIVITY NO - 2 - MycologysofiaNo ratings yet
- Kaotim MediKad Flyer ENDocument2 pagesKaotim MediKad Flyer ENUmm AbdullahNo ratings yet
- Medical Management of in Children: A Delphi Consensus: BlepharokeratoconjunctivitisDocument8 pagesMedical Management of in Children: A Delphi Consensus: Blepharokeratoconjunctivitisriskab123No ratings yet
- Blood Chemistry TestsDocument3 pagesBlood Chemistry TestsMarcelina ElizabethNo ratings yet
- Case Study - Ava LagambaDocument16 pagesCase Study - Ava Lagambaapi-717342251No ratings yet
- Review Article: The Spleen Revisited: An Overview On Magnetic Resonance ImagingDocument16 pagesReview Article: The Spleen Revisited: An Overview On Magnetic Resonance ImagingrusselioNo ratings yet
- Art Therapy For Individuals With Traumatic Brain Injury A Comprehensive Neurorehabilitation Informed Approach To TreatmentDocument8 pagesArt Therapy For Individuals With Traumatic Brain Injury A Comprehensive Neurorehabilitation Informed Approach To TreatmentCanela HeyNo ratings yet
- Psychiatric Drugs Are Neurotoxins-Power-Point-OutlineDocument30 pagesPsychiatric Drugs Are Neurotoxins-Power-Point-OutlineAugustaNo ratings yet
- SDL Abruptio Placenta Vs Placenta PreviaDocument3 pagesSDL Abruptio Placenta Vs Placenta PreviaVannesa TarifaNo ratings yet
- Wellness Massage LESSON 1-Plan The Wellness Program of ClientDocument7 pagesWellness Massage LESSON 1-Plan The Wellness Program of Clientma.fatima ravalo rabulanNo ratings yet
- Hepatitis BDocument23 pagesHepatitis BAbraham RumayaraNo ratings yet
- NICU DOH Compliance Monitoring Sheet 1Document2 pagesNICU DOH Compliance Monitoring Sheet 1Sherilyn RodriguezNo ratings yet
- Rotating TourniquetDocument3 pagesRotating TourniquetTom-tom LunaNo ratings yet
- FGH Preauthorization FormDocument1 pageFGH Preauthorization FormvijayNo ratings yet
- National Consumer Disputes Redressal Commission New Delhi Consumer Case No. 173 of 2011Document7 pagesNational Consumer Disputes Redressal Commission New Delhi Consumer Case No. 173 of 2011Arnav JoshiNo ratings yet
- Bipolar Disorder and Social Security Disability BenefitsDocument3 pagesBipolar Disorder and Social Security Disability BenefitsAndrew Egan100% (1)
- Pathophysiology of Portal Hypertension: Dr. Eeman At-Taras Dr. Mohamed Al-Saeid SulimanDocument29 pagesPathophysiology of Portal Hypertension: Dr. Eeman At-Taras Dr. Mohamed Al-Saeid SulimanDenata Prabhasiwi100% (1)
- 138296.folnegovi-Malc Et Al. - Farmakoterapija AB PDFDocument6 pages138296.folnegovi-Malc Et Al. - Farmakoterapija AB PDFIvanPrceNo ratings yet
- Department of Education: ScoreDocument3 pagesDepartment of Education: ScoreWilliamAporboNo ratings yet
- 1151 3608 1 PBDocument7 pages1151 3608 1 PBNilam SariNo ratings yet
- Going To The DoctorDocument4 pagesGoing To The DoctorJarod TempleNo ratings yet
- PATH505PDocument11 pagesPATH505PMohsin SialNo ratings yet
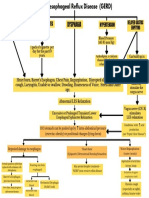
- Pathophysiology of Gastroesophageal Reflux (Gerd)Document1 pagePathophysiology of Gastroesophageal Reflux (Gerd)Joville DorueloNo ratings yet