You might also like
- Trauma HandbookDocument127 pagesTrauma Handbookarashkhan1No ratings yet
- First Aid Handbook: With Clear Explanations & 100+ Instructive ImagesFrom EverandFirst Aid Handbook: With Clear Explanations & 100+ Instructive ImagesNo ratings yet
- Mitral Valve Disease QuizDocument5 pagesMitral Valve Disease QuizReda SoNo ratings yet
- Aortic ExamDocument3 pagesAortic ExamReda SoNo ratings yet
- CCN (Critical Care Nursing)Document4 pagesCCN (Critical Care Nursing)Laurence ZernaNo ratings yet
- Clinical Assessment and Examination in OrthopedicsDocument196 pagesClinical Assessment and Examination in OrthopedicsMom of twoNo ratings yet
- AzSPU First Aid Management ProgrammeDocument12 pagesAzSPU First Aid Management ProgrammeAmir M. ShaikhNo ratings yet
- Greater Sydney Area HEMS Prehospital RSI ManualDocument20 pagesGreater Sydney Area HEMS Prehospital RSI ManualMiguel XanaduNo ratings yet
- NCP (Pre-Operative) : Assessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation Subjective CuesDocument2 pagesNCP (Pre-Operative) : Assessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation Subjective CuesYessamin100% (1)
- Shallo El Hard I90 BDocument2 pagesShallo El Hard I90 Belhard shalloNo ratings yet
- Tacloban City, Philippines 6500: Always Freque NT Sometim ES Seldo M Neve RDocument5 pagesTacloban City, Philippines 6500: Always Freque NT Sometim ES Seldo M Neve RMarc CalumpianoNo ratings yet
- 1 Triage NursingDocument28 pages1 Triage NursingRebecca FerolinoNo ratings yet
- Presented by Animesh Amal: Brand Plan On Salbutamol + Ambroxol + GuaifenesinDocument36 pagesPresented by Animesh Amal: Brand Plan On Salbutamol + Ambroxol + GuaifenesinAnonymous 75aETJ8ONo ratings yet
- Bagong Ospital NG Maynila Medical CenterDocument5 pagesBagong Ospital NG Maynila Medical CenterMary Patricia Tria100% (1)
- Code Blue ManagementDocument5 pagesCode Blue ManagementCorpus, Irene Zen P.No ratings yet
- Blunt Chest Trauma GuidelineDocument19 pagesBlunt Chest Trauma Guidelineana9filimonNo ratings yet
- Trauma Team RolesDocument12 pagesTrauma Team RolesaffanNo ratings yet
- KGH Code Blue Team RolesDocument5 pagesKGH Code Blue Team Rolesfanny_febrianiNo ratings yet
- Doc-20240131-Wa0 240131 224409Document6 pagesDoc-20240131-Wa0 240131 22440922alhumidi2020No ratings yet
- Team DynamicsDocument10 pagesTeam DynamicsNancy Jane TaguilingNo ratings yet
- Rural Acute Care SurgeryDocument37 pagesRural Acute Care SurgeryJOHANES BERECHMANS PRANOTO RUMARATUNo ratings yet
- Recavery After Anasthesia PDFDocument3 pagesRecavery After Anasthesia PDFYudionoNo ratings yet
- CPR Team DynamicsDocument31 pagesCPR Team Dynamicsapi-205902640No ratings yet
- Patient Recovery and Post-Anaesthesia Care Unit (PACU) : Learning ObjectivesDocument3 pagesPatient Recovery and Post-Anaesthesia Care Unit (PACU) : Learning ObjectivesnatashiaNo ratings yet
- Endorsement Clinical Handover/ EndorsementDocument4 pagesEndorsement Clinical Handover/ EndorsementGuiah RomaNo ratings yet
- Perioperative Nursing: Mammoplasty PlasticDocument10 pagesPerioperative Nursing: Mammoplasty PlasticMelanie GaledoNo ratings yet
- Wi-Qhse-0045 Rev 1 Merp Rev-1.Document20 pagesWi-Qhse-0045 Rev 1 Merp Rev-1.Isam AlasmoiNo ratings yet
- WK5 AclsDocument2 pagesWK5 AclsJhonny pingolNo ratings yet
- Quality and Safety Guidelines of Postanaesthesia CareDocument7 pagesQuality and Safety Guidelines of Postanaesthesia CareAdi CărbunaruNo ratings yet
- Red AlertDocument4 pagesRed AlertrositajarauNo ratings yet
- Nursing Code Blue PolicyDocument13 pagesNursing Code Blue PolicyQuennie Marie Moreno VillanuevaNo ratings yet
- POSITION PatientRestraintinEMSSystemsDocument6 pagesPOSITION PatientRestraintinEMSSystemsrisnayektiNo ratings yet
- Anaesthesia and Sedation Outside TheatresDocument15 pagesAnaesthesia and Sedation Outside Theatresمحمد زينNo ratings yet
- North Central Texas Trauma Regional Advisory CouncilDocument9 pagesNorth Central Texas Trauma Regional Advisory Councilashphoenix32No ratings yet
- 2015 LeeuwenbergDocument10 pages2015 LeeuwenbergPaulHerreraNo ratings yet
- Restraint Nursing Guideline For CareDocument9 pagesRestraint Nursing Guideline For Caresmith.kevin1420344No ratings yet
- Chain of Command ProcedureDocument7 pagesChain of Command ProceduresehrNo ratings yet
- Arrhythmias 2° To HyperkalaemiaDocument11 pagesArrhythmias 2° To Hyperkalaemiamarwanelsaeed1981No ratings yet
- Committee Opinion: Preparing For Clinical Emergencies in Obstetrics and GynecologyDocument3 pagesCommittee Opinion: Preparing For Clinical Emergencies in Obstetrics and GynecologyMochammad Rizal AttamimiNo ratings yet
- Clinical Practice Guidelines - Protocols - July 2018Document229 pagesClinical Practice Guidelines - Protocols - July 2018Muzi SitholeNo ratings yet
- Code Blue System: Nursing Perspectives: Cirebon City West Java IndonesiaDocument24 pagesCode Blue System: Nursing Perspectives: Cirebon City West Java Indonesiaade asri damayanti100% (1)
- Standard operating procedure for collapsed inpatientsDocument6 pagesStandard operating procedure for collapsed inpatientsAnggriawanCaesarNurfattah100% (1)
- Basic Life Suppor T: Monalyn B. La-Ao, RN Glenn Ryan Palao-Ay, RNDocument37 pagesBasic Life Suppor T: Monalyn B. La-Ao, RN Glenn Ryan Palao-Ay, RNMarlon Pilis B CanggatNo ratings yet
- Early Mobility Care GuidelineDocument7 pagesEarly Mobility Care GuidelineAny AndrianiNo ratings yet
- Standard Treatment ProtolsDocument80 pagesStandard Treatment ProtolsMauzoom AliNo ratings yet
- COP EmergencyDocument15 pagesCOP EmergencyOyinlola EbenezerNo ratings yet
- Code Blue Team: Roles and Function: Stage 1: Activation PhaseDocument5 pagesCode Blue Team: Roles and Function: Stage 1: Activation PhaseRero CitroNo ratings yet
- Amores Reviewer Ko GawaDocument12 pagesAmores Reviewer Ko GawaBryant Von Andrew EstradaNo ratings yet
- Maximizing Success With Rapid Sequence IntubationsDocument11 pagesMaximizing Success With Rapid Sequence IntubationsRaymond RosarioNo ratings yet
- 06 Materi Post PerioperativeDocument12 pages06 Materi Post PerioperativeRino SetiadyNo ratings yet
- Spinal Cord Injury Pathway AlgorithmDocument13 pagesSpinal Cord Injury Pathway Algorithmnurul ismaniaNo ratings yet
- Rcs e v13 With Guidelines Score SheetDocument4 pagesRcs e v13 With Guidelines Score SheetgabrimarteNo ratings yet
- Ipd Documentation Jr'sDocument12 pagesIpd Documentation Jr'sQuality AIIMSUdrNo ratings yet
- Advanced Cardiovascular Life SupportDocument16 pagesAdvanced Cardiovascular Life SupportSarah Mohd YusofNo ratings yet
- Waiters Proning PDFDocument1 pageWaiters Proning PDFmp1757No ratings yet
- MdLuvw-UnknownDocument42 pagesMdLuvw-Unknownmohammed ahmedNo ratings yet
- F 1177 - 96 - Rjexnzctotzb PDFDocument3 pagesF 1177 - 96 - Rjexnzctotzb PDFqmsudhirNo ratings yet
- Cardiopulmonary Resuscitation (CPR) Policy: Associated DocumentsDocument24 pagesCardiopulmonary Resuscitation (CPR) Policy: Associated DocumentsNur SusiawantyNo ratings yet
- ICU patient transfer guidelineDocument8 pagesICU patient transfer guidelineInnas DoankNo ratings yet
- Cec Post Fall Assess and Man June 2013Document3 pagesCec Post Fall Assess and Man June 2013Vicente TurasNo ratings yet
- ERC 2015 Basic Life SupportDocument19 pagesERC 2015 Basic Life SupportfentaNo ratings yet
- Emergency NursingDocument2 pagesEmergency NursingJUDE MARIANO JR. ALBANCES CARLOSNo ratings yet
- Intubation of Sick Children - Practical Tips For Adult Intensivists Anaesthesia Tutorial of The Week 169 8 February 2010Document10 pagesIntubation of Sick Children - Practical Tips For Adult Intensivists Anaesthesia Tutorial of The Week 169 8 February 2010khalidNo ratings yet
- Emergency Trolley GuidelineDocument3 pagesEmergency Trolley GuidelineNur SusiawantyNo ratings yet
- Arc Guideline 11 1 Introduction To and Principles of in Hospital Resuscitation Feb 2019Document22 pagesArc Guideline 11 1 Introduction To and Principles of in Hospital Resuscitation Feb 2019hernandez2812No ratings yet
- Cream Pastel Palette Healthcare Center CharactersDocument138 pagesCream Pastel Palette Healthcare Center CharactersFlourence ZafranNo ratings yet
- Chinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Document11 pagesChinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Reda SoNo ratings yet
- CHAPTER 55 - Percutaneous Coronary InterventionDocument1 pageCHAPTER 55 - Percutaneous Coronary InterventionReda SoNo ratings yet
- Ward Reflection PaperDocument1 pageWard Reflection PaperReda SoNo ratings yet
- Answer Key-Mitral ValveDocument6 pagesAnswer Key-Mitral ValveReda SoNo ratings yet
- Chapter 32 - Genetic Cardiac ArrythmiasDocument7 pagesChapter 32 - Genetic Cardiac ArrythmiasReda SoNo ratings yet
- Risk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Document7 pagesRisk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Reda SoNo ratings yet
- Braunwald Chapter KeypointersDocument6 pagesBraunwald Chapter KeypointersReda SoNo ratings yet
- CHAPTER 27 - Heart Failure With A Preserved Ejection FractionDocument15 pagesCHAPTER 27 - Heart Failure With A Preserved Ejection FractionReda SoNo ratings yet
- CH 50 - Approach To Patient With Chest PainDocument1 pageCH 50 - Approach To Patient With Chest PainReda SoNo ratings yet
- Name: - Year LevelDocument6 pagesName: - Year LevelReda SoNo ratings yet
- Private Ward Admission Census 1Document6 pagesPrivate Ward Admission Census 1Reda SoNo ratings yet
- Evidence-Based Approach to Heart Failure History and Physical ExamDocument5 pagesEvidence-Based Approach to Heart Failure History and Physical ExamReda SoNo ratings yet
- Tilt Table Testing: Name Age/Sex APDocument1 pageTilt Table Testing: Name Age/Sex APReda SoNo ratings yet
- Coronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Document3 pagesCoronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Reda SoNo ratings yet
- Trials SummaryDocument12 pagesTrials SummaryReda SoNo ratings yet
- CHAPTER 61: Diabetes and The Cardiovascular System: Ma. Arnee V. Anico-Tondo, M.D., FPCP (CGH)Document1 pageCHAPTER 61: Diabetes and The Cardiovascular System: Ma. Arnee V. Anico-Tondo, M.D., FPCP (CGH)Reda SoNo ratings yet
- Coronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Document3 pagesCoronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Reda SoNo ratings yet
- Vascular Conference: JUNE 2018 - MARCH 2019Document2 pagesVascular Conference: JUNE 2018 - MARCH 2019Reda SoNo ratings yet
- Cardiology census and patient detailsDocument9 pagesCardiology census and patient detailsReda SoNo ratings yet
- Heart Institute Team Building April 2019Document1 pageHeart Institute Team Building April 2019Reda SoNo ratings yet
- Marijuana LegalizationDocument5 pagesMarijuana LegalizationMatt ImpellusoNo ratings yet
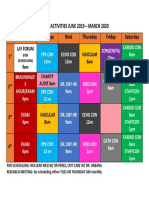
- Daily Activities 2019Document1 pageDaily Activities 2019Reda SoNo ratings yet
- Tilt Table Testing: Name Age/Sex APDocument1 pageTilt Table Testing: Name Age/Sex APReda SoNo ratings yet
- Computed Tomography Findings for 8 Cardiovascular PatientsDocument1 pageComputed Tomography Findings for 8 Cardiovascular PatientsReda SoNo ratings yet
- 2011 PadDocument19 pages2011 PadReda SoNo ratings yet
- Case Protocol 3Document5 pagesCase Protocol 3Reda SoNo ratings yet
- Case Protocol 3Document2 pagesCase Protocol 3Reda SoNo ratings yet
- HRH Data Mapping TemplateDocument24 pagesHRH Data Mapping TemplateJohn DanielNo ratings yet
- EEReview PDFDocument7 pagesEEReview PDFragavendharNo ratings yet
- B36 Group 6 Community Engagement ProposalDocument5 pagesB36 Group 6 Community Engagement ProposalLenard SusanoNo ratings yet
- Adrian Castelan Resume 3Document2 pagesAdrian Castelan Resume 3api-532744620No ratings yet
- Prof. Erica Wood - APEC PBMDocument46 pagesProf. Erica Wood - APEC PBMbudi darmantaNo ratings yet
- Simplified MELC-Based Budget of Lesson in Animal Production (Swine) NC IIDocument5 pagesSimplified MELC-Based Budget of Lesson in Animal Production (Swine) NC IImichael hobayanNo ratings yet
- Treating Two Adjacent Missing Teeth in The Esthetic ZoneDocument13 pagesTreating Two Adjacent Missing Teeth in The Esthetic ZonetastykNo ratings yet
- The Open Dentistry Journal: The Effect of Chin-Cup Therapy in Class III Malocclusion: A Systematic ReviewDocument16 pagesThe Open Dentistry Journal: The Effect of Chin-Cup Therapy in Class III Malocclusion: A Systematic ReviewmilanmashrukNo ratings yet
- Gambian DHS 2019-20Document4 pagesGambian DHS 2019-20josetelhadoNo ratings yet
- Running Head: Elements of An Organizational Model of Health CareDocument7 pagesRunning Head: Elements of An Organizational Model of Health Careklm klmNo ratings yet
- Suven Life Sciences Secures Three (3) Product Patents in Canada, ARIPO and South Korea (Company Update)Document2 pagesSuven Life Sciences Secures Three (3) Product Patents in Canada, ARIPO and South Korea (Company Update)Shyam SunderNo ratings yet
- Clinical EpidemiologyDocument38 pagesClinical EpidemiologyLilis Tuslinah100% (1)
- PBRL 420 Unilever Media KitDocument8 pagesPBRL 420 Unilever Media Kitapi-650275339No ratings yet
- Prevalence and Incidence of Rheumatoid Arthritis in Italy: Original ArticleDocument6 pagesPrevalence and Incidence of Rheumatoid Arthritis in Italy: Original ArticleDiego Francesco MacaliNo ratings yet
- Final Oral Health Resource May 2011 Web Version PDFDocument137 pagesFinal Oral Health Resource May 2011 Web Version PDFvyaa primasariNo ratings yet
- NCP Cva Ineffective Tissue PerfusionDocument1 pageNCP Cva Ineffective Tissue PerfusionNina Glaiza Goto100% (1)
- ID Identifikasi Listeria Monocytogenes Pada PDFDocument8 pagesID Identifikasi Listeria Monocytogenes Pada PDFRiani AniNo ratings yet
- Open Letter To AASDDocument4 pagesOpen Letter To AASDWBAYNo ratings yet
- Notification Letter EnglishDocument1 pageNotification Letter EnglishJovele OctobreNo ratings yet
- MIDWIFERY AND OBSTETRICAL CAREDocument92 pagesMIDWIFERY AND OBSTETRICAL CARESanthosh.S.UNo ratings yet
- BBBFDocument3 pagesBBBFSkAliHassanNo ratings yet
- Results of HSRC Study On South African Healthcare Workers Mental Health and Covid 19Document64 pagesResults of HSRC Study On South African Healthcare Workers Mental Health and Covid 19Laura Lopez GonzalezNo ratings yet
- AO CMFS During COVID-19Document6 pagesAO CMFS During COVID-19โสภาพรรณวดี รวีวารNo ratings yet
- Post Dural Puncture HeadacheDocument7 pagesPost Dural Puncture Headachedrsaurav86623No ratings yet