You might also like
- Tomita2019 Article Self-expandableMetallicStentinDocument11 pagesTomita2019 Article Self-expandableMetallicStentinSisca Dwi AgustinaNo ratings yet
- Rekap Operasi ONKO Selama Covid-19Document8 pagesRekap Operasi ONKO Selama Covid-19Sisca Dwi AgustinaNo ratings yet
- Clinical Interpretation of Elevated CA 19-9 Levels in Obstructive Jaundice Following Benign and Malignant Pancreatobiliary DiseaseDocument7 pagesClinical Interpretation of Elevated CA 19-9 Levels in Obstructive Jaundice Following Benign and Malignant Pancreatobiliary DiseaseSisca Dwi AgustinaNo ratings yet
- The Effects of Different Suture Techniques On Wound Healing in Abdominal Wall ClosureDocument4 pagesThe Effects of Different Suture Techniques On Wound Healing in Abdominal Wall ClosureSisca Dwi AgustinaNo ratings yet
- Safety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaDocument9 pagesSafety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaSisca Dwi AgustinaNo ratings yet
- Immunohistochemically Detected Expression of 3 Major Genes (CDKN2A/p16, TP53, and SMAD4/DPC4) Strongly Predicts Survival in Patients With Resectable Pancreatic CancerDocument11 pagesImmunohistochemically Detected Expression of 3 Major Genes (CDKN2A/p16, TP53, and SMAD4/DPC4) Strongly Predicts Survival in Patients With Resectable Pancreatic CancerSisca Dwi AgustinaNo ratings yet
- Update Laporan Jaga II Onkologi Minggu II SeptemberDocument12 pagesUpdate Laporan Jaga II Onkologi Minggu II SeptemberSisca Dwi AgustinaNo ratings yet
- Endovascular Versus Surgical Revascularization For Acute Limb IschemiaDocument9 pagesEndovascular Versus Surgical Revascularization For Acute Limb IschemiaSisca Dwi AgustinaNo ratings yet
- 10.1007@s00268 012 1745 3Document6 pages10.1007@s00268 012 1745 3Sisca Dwi AgustinaNo ratings yet
- Case Rreport Ameloblastoma English1Document13 pagesCase Rreport Ameloblastoma English1Sisca Dwi AgustinaNo ratings yet
- Perioperative Blood TransfusionDocument4 pagesPerioperative Blood TransfusionSisca Dwi AgustinaNo ratings yet
- Molecular Biology of Wound Healing: Ental Science - Short CommunicationDocument5 pagesMolecular Biology of Wound Healing: Ental Science - Short CommunicationSisca Dwi AgustinaNo ratings yet
- Preventing Contrast-Induced Renal Failure: A Guide: CoronaryDocument7 pagesPreventing Contrast-Induced Renal Failure: A Guide: CoronarySisca Dwi AgustinaNo ratings yet
- SOCC NCE FullProgramDocument56 pagesSOCC NCE FullProgramSisca Dwi AgustinaNo ratings yet
- Indian J Derma To L Cross SectionalDocument5 pagesIndian J Derma To L Cross SectionalSisca Dwi AgustinaNo ratings yet
- 4d85 PDFDocument4 pages4d85 PDFSisca Dwi AgustinaNo ratings yet
- Outcome of Intensive Care Unit Patients Using Pediatric Risk of Mortality (PRISM) ScoreDocument2 pagesOutcome of Intensive Care Unit Patients Using Pediatric Risk of Mortality (PRISM) ScoreSisca Dwi AgustinaNo ratings yet
- UptodateDocument21 pagesUptodateSisca Dwi AgustinaNo ratings yet
- Current Options in Umbilical Hernia Repair in Adult PatientsDocument5 pagesCurrent Options in Umbilical Hernia Repair in Adult PatientsSisca Dwi AgustinaNo ratings yet
- Practice Guidelines For Perioperative Blood Management PDFDocument35 pagesPractice Guidelines For Perioperative Blood Management PDFbeautifulbeastNo ratings yet
- Association of Voiding Dysfunction With Functional ConstipationDocument3 pagesAssociation of Voiding Dysfunction With Functional ConstipationSisca Dwi AgustinaNo ratings yet
- Ismaeil 2018Document15 pagesIsmaeil 2018Javier ZaquinaulaNo ratings yet
- Wound Management ProcedureDocument51 pagesWound Management ProcedureSisca Dwi AgustinaNo ratings yet
- Baumann 2018Document13 pagesBaumann 2018Sisca Dwi AgustinaNo ratings yet
- Smad4 Loss Enables Egf, Tgfβ1 And S100A8/A9 Induced Activation Of Critical Pathways To Invasion In Human Pancreatic Adenocarcinoma CellsDocument18 pagesSmad4 Loss Enables Egf, Tgfβ1 And S100A8/A9 Induced Activation Of Critical Pathways To Invasion In Human Pancreatic Adenocarcinoma CellsSisca Dwi AgustinaNo ratings yet
- Daftar PustakaDocument1 pageDaftar PustakaSisca Dwi AgustinaNo ratings yet
- Perioperative Blood TransfusionDocument4 pagesPerioperative Blood TransfusionSisca Dwi AgustinaNo ratings yet
- The Open Dentistry JournalDocument10 pagesThe Open Dentistry JournalSisca Dwi AgustinaNo ratings yet
- Fast Growing Jaw Osteosarcoma in A 55 Year Old Womana Case ReportDocument4 pagesFast Growing Jaw Osteosarcoma in A 55 Year Old Womana Case ReportSisca Dwi AgustinaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Sepsis 2021 A ReviewDocument9 pagesSepsis 2021 A ReviewvictorNo ratings yet
- NREMT Study Guide ProjectDocument12 pagesNREMT Study Guide ProjectGabriel SionsNo ratings yet
- First Aid QuizDocument2 pagesFirst Aid QuizMichellene Tadle100% (1)
- Blood VesselsDocument16 pagesBlood VesselsAlen OsmanovicNo ratings yet
- Cardiovascular ExamDocument11 pagesCardiovascular ExamDonndulf Tizon Maningas100% (1)
- Thesis On Nursing DocumentationDocument5 pagesThesis On Nursing DocumentationJennifer Strong100% (2)
- Surviving Sepsis Campaign 2016 Guidelines Presentation Final RevisiedDocument32 pagesSurviving Sepsis Campaign 2016 Guidelines Presentation Final RevisiedAdli Wafi Jabbar100% (1)
- Fccs Course Administration: Licensed Activities PortalDocument8 pagesFccs Course Administration: Licensed Activities PortalRizki Baiti OktaviyaniNo ratings yet
- Study Guide NREMTDocument4 pagesStudy Guide NREMTdebbiemedic355740% (5)
- Inflammatory Response in Cardiovascular Surgery 2013Document432 pagesInflammatory Response in Cardiovascular Surgery 2013Rodrigo Villanova BrasilNo ratings yet
- Dwnload Full Nursing A Concept Based Approach To Learning Volume 1 2nd Edition Pearson Test Bank PDFDocument36 pagesDwnload Full Nursing A Concept Based Approach To Learning Volume 1 2nd Edition Pearson Test Bank PDFmichaelcalhounjtypaegbnk100% (11)
- NCM 106 - ABCDE AssessmentDocument35 pagesNCM 106 - ABCDE Assessmentエルミタ ジョイ ファティマNo ratings yet
- MOHAN Di. RAJU....... MOHAN Di. RAJU......Document32 pagesMOHAN Di. RAJU....... MOHAN Di. RAJU......Nagaraja ReddyNo ratings yet
- Nurse EcmoDocument124 pagesNurse EcmoSalvatore Cimino100% (5)
- Assessment of Fluid Responsiveness Recent Advances. OkDocument6 pagesAssessment of Fluid Responsiveness Recent Advances. OkLeiniker Navarro Rey100% (1)
- Sepsis Nursing OutlineDocument6 pagesSepsis Nursing OutlineSavannah Hayden100% (1)
- Guía Manejo Del Shock 2023Document67 pagesGuía Manejo Del Shock 2023Alvaro ArriagadaNo ratings yet
- Gastric Ulcer Nursing CareDocument6 pagesGastric Ulcer Nursing CareAesthea BondadNo ratings yet
- The Pediatrics HO GuideDocument44 pagesThe Pediatrics HO GuideAlex MatthewNo ratings yet
- Chapter 4 - Mixed Venous Oxygen SaturationDocument3 pagesChapter 4 - Mixed Venous Oxygen SaturationJamesNo ratings yet
- Sepsis Syndromes: PrinciplesDocument11 pagesSepsis Syndromes: PrinciplesdiludipaNo ratings yet
- ER Nurse ChecklistDocument3 pagesER Nurse Checklistdocpanchu100% (1)
- ShockDocument33 pagesShockVijith.V.kumarNo ratings yet
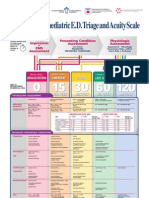
- Paediatric Triage PosterDocument1 pagePaediatric Triage PosterGenaro Olmos Garcia100% (2)
- AIIMS Delhi Nursing Officer Exam 2019 Memory Based Question Paper SummaryDocument40 pagesAIIMS Delhi Nursing Officer Exam 2019 Memory Based Question Paper Summaryrejin rejinrNo ratings yet
- ACLS 2012 Pre-TesteDocument14 pagesACLS 2012 Pre-TesteVitor Hugo G Correia100% (9)
- 75 Items Practice ExamDocument42 pages75 Items Practice ExamTed ChrisNo ratings yet
- Surgery Surgical Nursing Objs With AnsDocument136 pagesSurgery Surgical Nursing Objs With AnsmintahmeshackbenjaminNo ratings yet
- Perioperative Nursing CareDocument47 pagesPerioperative Nursing CareTessa Bagus AriyantoNo ratings yet
- Azam IndexDocument7 pagesAzam IndexBiswajitNo ratings yet