You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Soal TO AIPKIDocument45 pagesSoal TO AIPKIrosalina80% (5)
- Newton Fund Institutional Links Grants - Application (2018 IL7 - April)Document31 pagesNewton Fund Institutional Links Grants - Application (2018 IL7 - April)Marzuki Panji WijayaNo ratings yet
- Guias Hemorragia PospartoDocument48 pagesGuias Hemorragia PospartoDai UmqandmcNo ratings yet
- Paris PDFDocument44 pagesParis PDFMarzuki Panji WijayaNo ratings yet
- WHO Dengue Hemorrhagic Fever Diagnosis, Treatment, Prevention and Control 1997Document0 pagesWHO Dengue Hemorrhagic Fever Diagnosis, Treatment, Prevention and Control 1997Maryam JamilahNo ratings yet
- Venous Function and Central Venous Pressure: A Physiologic StoryDocument14 pagesVenous Function and Central Venous Pressure: A Physiologic StoryMarzuki Panji WijayaNo ratings yet
- IV In-Line Filters CochraneDocument19 pagesIV In-Line Filters CochraneMarzuki Panji WijayaNo ratings yet
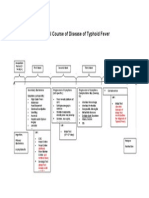
- Natural Course of Disease of Typhoid FeverDocument1 pageNatural Course of Disease of Typhoid FeverMarzuki Panji WijayaNo ratings yet
- Diabetes Education BookletDocument11 pagesDiabetes Education BookletMarzuki Panji WijayaNo ratings yet
- Diabetes Education BookletDocument11 pagesDiabetes Education BookletMarzuki Panji WijayaNo ratings yet
- BetahistineDocument8 pagesBetahistineJohn Michael ValienteNo ratings yet
- Insulin GlargineDocument1 pageInsulin GlargineNelson GoulartNo ratings yet
- McCance Patho Review QsDocument17 pagesMcCance Patho Review Qsiamdara100% (1)
- Turners Syndrome: Sonika Shimon Prasad S160232Document20 pagesTurners Syndrome: Sonika Shimon Prasad S160232Ivy DanNo ratings yet
- Prediction of Stroke Using Machine Learning: June 2020Document10 pagesPrediction of Stroke Using Machine Learning: June 2020Musaddique DangeNo ratings yet
- Mini-OSCE Internal PicturesDocument108 pagesMini-OSCE Internal PicturesCheru TadesseNo ratings yet
- Atypical Facial PainDocument5 pagesAtypical Facial PainRenju KuriakoseNo ratings yet
- Subject: Leukemia Professor: Ia Marashkhia Researcher: Alireza Farhadiyeh (1701940)Document14 pagesSubject: Leukemia Professor: Ia Marashkhia Researcher: Alireza Farhadiyeh (1701940)alirezaNo ratings yet
- Case 1 AbortionDocument18 pagesCase 1 AbortionEduard GarchitorenaNo ratings yet
- Gynera: Coated TabletsDocument67 pagesGynera: Coated TabletsOdeke VascoNo ratings yet
- Comparing Ultra-Hypofractionated Proton Versus Photon Therapy in Extremity Soft Tissue SarcomaDocument10 pagesComparing Ultra-Hypofractionated Proton Versus Photon Therapy in Extremity Soft Tissue SarcomaRaul Matute MartinNo ratings yet
- Narrative ReportDocument1 pageNarrative ReportMelvin Aurelio100% (1)
- Universidad Santiago de CaliDocument3 pagesUniversidad Santiago de CaliValentina MorenoNo ratings yet
- Thyroid Diseases: Peter S. Aznar, MD, FPSP, MhpeDocument52 pagesThyroid Diseases: Peter S. Aznar, MD, FPSP, MhpeDeomicah SolanoNo ratings yet
- COPD PathophysioDocument1 pageCOPD Pathophysionanette flores dela cruzNo ratings yet
- Medication Information For Parents and Teachers: Guanfacine-Tenex, IntunivDocument8 pagesMedication Information For Parents and Teachers: Guanfacine-Tenex, IntunivMonique Wright100% (1)
- Krok I 2013-17 ExplainedDocument292 pagesKrok I 2013-17 ExplainedU1GoKu0% (1)
- Sleep Disorder Screening ToolDocument2 pagesSleep Disorder Screening ToolVivek TiwariNo ratings yet
- Name: Lufty Meisya Alfileri Class: X-2Document3 pagesName: Lufty Meisya Alfileri Class: X-2Fida TsabitaNo ratings yet
- Urology Case Reports: Abdullah, Junping XingDocument3 pagesUrology Case Reports: Abdullah, Junping XingHardiTariqHammaNo ratings yet
- CMT 05210 Internal MedicineDocument23 pagesCMT 05210 Internal MedicineBashiru SelemaniNo ratings yet
- Poisonplants 140917075435 Phpapp02 PDFDocument42 pagesPoisonplants 140917075435 Phpapp02 PDFNareshNo ratings yet
- X-Ray Interpretation Skills: Dr. Hisham AlsanawiDocument68 pagesX-Ray Interpretation Skills: Dr. Hisham AlsanawiVika DamayNo ratings yet
- Example of Completed Blood Safety Indicators FormDocument9 pagesExample of Completed Blood Safety Indicators FormEmhemed Amer TabibNo ratings yet
- Pityriasis AmiantaceaDocument4 pagesPityriasis AmiantaceaWidia WidiaaNo ratings yet
- 8 Effective Acupressure Points For Lungs Recommended by TCM Practitioners - TCM TipsDocument25 pages8 Effective Acupressure Points For Lungs Recommended by TCM Practitioners - TCM TipsCarl MacCordNo ratings yet
- Pathognomonic SignsDocument4 pagesPathognomonic SignsJoan Rose Rendon-Hung50% (2)
- Erbs Palsy PDFDocument4 pagesErbs Palsy PDFKamran AfzalNo ratings yet
- First Degree BurnsDocument3 pagesFirst Degree BurnsbobboxNo ratings yet
- Sgot & SGPTDocument2 pagesSgot & SGPT우영박No ratings yet