You might also like
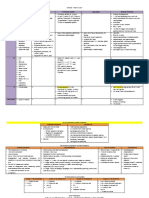
- The 3rd Year Derma Missing TableDocument6 pagesThe 3rd Year Derma Missing TableEmil GulmaticoNo ratings yet
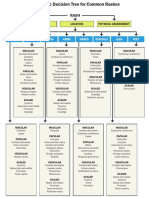
- WK 5 Rash Decision TreeDocument1 pageWK 5 Rash Decision TreeBetsy Brown ByersmithNo ratings yet
- Derm StuffDocument7 pagesDerm StuffSudesna Roy ChowdhuryNo ratings yet
- Handbook of Skin DiseasesDocument43 pagesHandbook of Skin DiseasesTrixDelaCruzNo ratings yet
- Basic Skin Lesions: Presented By: Dr. Divyank A. Vankawala Jr. Resident, Dermatology Dept., NDMVPS VP Medical CollegeDocument46 pagesBasic Skin Lesions: Presented By: Dr. Divyank A. Vankawala Jr. Resident, Dermatology Dept., NDMVPS VP Medical CollegeniveditakartikNo ratings yet
- Basic Lesions: Dr. Mahroof ThamarasseryDocument58 pagesBasic Lesions: Dr. Mahroof ThamarasseryYasmin DworkNo ratings yet
- PsoriasisDocument27 pagesPsoriasisMishaNo ratings yet
- Internal Medicine Finals ReviewerDocument8 pagesInternal Medicine Finals ReviewerRojales FrancisNo ratings yet
- Anal and Perianal ConditionsDocument58 pagesAnal and Perianal ConditionsYonas YemidiralemNo ratings yet
- Scrotal MassesDocument19 pagesScrotal MassesJohnNo ratings yet
- Introduction To SkinDocument60 pagesIntroduction To SkinAleena MalikNo ratings yet
- Psoriasis: For Health Officer Students Solomon H (MD, DVR)Document38 pagesPsoriasis: For Health Officer Students Solomon H (MD, DVR)Theo Grazila RuvaNo ratings yet
- Lichen PlanusDocument17 pagesLichen PlanusRahma Tya Anwar0% (1)
- 547 2094 1 PB PDFDocument8 pages547 2094 1 PB PDFYesichaNo ratings yet
- Ent Diseases of The Oral and Pharynx Dr. UyDocument7 pagesEnt Diseases of The Oral and Pharynx Dr. UyAileen EmyNo ratings yet
- Skin DiseasesDocument11 pagesSkin DiseasesPipoy Amy100% (1)
- Fungal InfectionsDocument9 pagesFungal InfectionsCoral Srinivasa RamaluNo ratings yet
- Derm ChartDocument109 pagesDerm ChartAlana BolloneNo ratings yet
- Anti FUNGAL Drugs PDFDocument70 pagesAnti FUNGAL Drugs PDFHester Marie SimpiaNo ratings yet
- Psoriasis Dermatitis FinalDocument50 pagesPsoriasis Dermatitis Finalapi-546809761No ratings yet
- Arya. Skin Path LabDocument54 pagesArya. Skin Path LabMJO79No ratings yet
- Superficial and Deep Perivascular DermatitisDocument55 pagesSuperficial and Deep Perivascular DermatitisMarnie RoviraNo ratings yet
- PSORIASISDocument27 pagesPSORIASISnurulzakinahnunu100% (1)
- Skin Infections and InfestationsDocument37 pagesSkin Infections and InfestationsAremu OlatayoNo ratings yet
- Hernia and Perianal ConditionsDocument58 pagesHernia and Perianal ConditionsSocial Media workingNo ratings yet
- Pulmo Case Simulation-TEAM Yellow-Blue - 01-04-21Document35 pagesPulmo Case Simulation-TEAM Yellow-Blue - 01-04-21Jolaine ValloNo ratings yet
- Introduction To Dermatology Assessment of A Dermatologic PatientDocument86 pagesIntroduction To Dermatology Assessment of A Dermatologic PatientAtifNo ratings yet
- Spongiotic Dermatitis: Aka EczemaDocument8 pagesSpongiotic Dermatitis: Aka EczemafadoNo ratings yet
- Dermatology OSCE Pictures 1Document208 pagesDermatology OSCE Pictures 1medt80No ratings yet
- Traditional Ayurvedic Medicines Pathway To Develop Anticancer Drugs 2329 9053 1000130Document11 pagesTraditional Ayurvedic Medicines Pathway To Develop Anticancer Drugs 2329 9053 1000130shiva_99No ratings yet
- Histology by - Dr.abdirahman Gagajir 1Document40 pagesHistology by - Dr.abdirahman Gagajir 1HusseinNo ratings yet
- SkinDocument8 pagesSkinkuu faalNo ratings yet
- Physical Trauma (Koebner's Phenomenon) Is A Major Factor in Eliciting LesionsDocument12 pagesPhysical Trauma (Koebner's Phenomenon) Is A Major Factor in Eliciting LesionsNaomi AnastacioNo ratings yet
- Hem-Onc: AnswerDocument3 pagesHem-Onc: AnswerAman Raj KNo ratings yet
- Disorders of Sweat and Sebaceous GlandsDocument43 pagesDisorders of Sweat and Sebaceous GlandsSantosh ThapaNo ratings yet
- Acne Vulgaris Acne Rosacea Acne Disorders: Systemic Lupus ErythematosusDocument19 pagesAcne Vulgaris Acne Rosacea Acne Disorders: Systemic Lupus Erythematosusapi-26938624No ratings yet
- Erythema MultiformeDocument29 pagesErythema MultiformeSurabhi Sharma100% (1)
- West Notes-1 PDFDocument17 pagesWest Notes-1 PDFSerious LeoNo ratings yet
- Dermatology Lectures JRRMMCDocument10 pagesDermatology Lectures JRRMMCGi Em100% (1)
- Dengue Virus: DescriptionDocument12 pagesDengue Virus: Descriptionpedia blue bookNo ratings yet
- Negations in Mullukurumba and Kattunaikka Tribes in NilgirisDocument5 pagesNegations in Mullukurumba and Kattunaikka Tribes in NilgirisEditor IJTSRDNo ratings yet
- (Warding) Guideline 1 - QCGH-HISTORY - PE - GUIDELINEDocument4 pages(Warding) Guideline 1 - QCGH-HISTORY - PE - GUIDELINEHynne Jhea Echavez100% (1)
- Internal Medicine Quick TablesDocument276 pagesInternal Medicine Quick Tablesjoey plouffeNo ratings yet
- # Diseases of ConjunctivaDocument4 pages# Diseases of Conjunctivaameerabest100% (1)
- Dermatology - LoveDocument433 pagesDermatology - LoveAntonio EscobarNo ratings yet
- Review Slides OphthaDocument14 pagesReview Slides OphthaSUSHMITA MAE ROSE CONTRERASNo ratings yet
- Derm Pathology PDFDocument21 pagesDerm Pathology PDFMara MitrutNo ratings yet
- PnemoniaDocument4 pagesPnemoniadhavalNo ratings yet
- 01-05-21 - 01-12-21 - Fluid & ElectrolytesDocument8 pages01-05-21 - 01-12-21 - Fluid & ElectrolytesJolaine ValloNo ratings yet
- Anemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDocument15 pagesAnemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDanielle FosterNo ratings yet
- Skin PathogensDocument4 pagesSkin PathogensEhi EdialeNo ratings yet
- Anti Fungal DrugsDocument6 pagesAnti Fungal Drugsbilal ahmadNo ratings yet
- Bacterial Skin Infections - Course VIIIDocument37 pagesBacterial Skin Infections - Course VIIIAngelie PedregosaNo ratings yet
- Shanz - Pedia Ii 2.05Document3 pagesShanz - Pedia Ii 2.05Petrina XuNo ratings yet
- Superficial Fungal Infections of The Skin VoiceoverDocument67 pagesSuperficial Fungal Infections of The Skin VoiceoverMedo JT100% (1)
- Dse Pathogenesis/ Causes Diagnosis Complications TX Prognosis NotesDocument5 pagesDse Pathogenesis/ Causes Diagnosis Complications TX Prognosis NotesLuka Desabelle- JustoNo ratings yet
- Ecological Study of Seabuckthorn (Hippophae L.) in Mustang and Manang Districts, NepalDocument8 pagesEcological Study of Seabuckthorn (Hippophae L.) in Mustang and Manang Districts, Nepalkhilendra gurungNo ratings yet
- External Ear DiseasesDocument6 pagesExternal Ear DiseasesJohn Christopher LucesNo ratings yet
- Lesi Kulit & Pemeriksaan LaboratoriumDocument129 pagesLesi Kulit & Pemeriksaan LaboratoriumUmitha Rahmi SaniNo ratings yet
- Power Point Week #3Document182 pagesPower Point Week #3Raelene MarceauNo ratings yet
- Pedia - History Taking and Physical Exam - PGI Leira BarbosaDocument6 pagesPedia - History Taking and Physical Exam - PGI Leira BarbosaLeira BarbosaNo ratings yet
- Ospital NG Maynila Medical Center: Department of SurgeryDocument6 pagesOspital NG Maynila Medical Center: Department of SurgeryLeira BarbosaNo ratings yet
- Gallstones in Pregnancy - UpToDateDocument51 pagesGallstones in Pregnancy - UpToDateLeira BarbosaNo ratings yet
- MapehDocument31 pagesMapehLeira BarbosaNo ratings yet
- Blisters Read Only RVDocument75 pagesBlisters Read Only RVFrederica MutiaraNo ratings yet
- Summary of DermaDocument29 pagesSummary of DermaAbdelrahman ElsaadawiNo ratings yet
- Bacterial Infections of Human ProjectDocument29 pagesBacterial Infections of Human ProjectCute AkoNo ratings yet
- Cues Nursing Diagnosis Analysis Goal Intervention Rationale EvaluationDocument19 pagesCues Nursing Diagnosis Analysis Goal Intervention Rationale EvaluationEmeEmeka100% (1)
- Notes Skin Eye Ears Infections MicrobioDocument18 pagesNotes Skin Eye Ears Infections MicrobioChristiel John MagtibayNo ratings yet
- Disorders of Skin in ChildrenDocument47 pagesDisorders of Skin in Childrensmriti boraNo ratings yet
- Management of Common Infections With Antimicrobials Guidance Clinical Practice Guidelines (2019) PDFDocument4 pagesManagement of Common Infections With Antimicrobials Guidance Clinical Practice Guidelines (2019) PDFveerrajuNo ratings yet
- Impetigo PDFDocument7 pagesImpetigo PDFdestraNo ratings yet
- PYODERMADocument45 pagesPYODERMAAiman Tymer80% (5)
- Dermatologic DiseaseDocument31 pagesDermatologic Diseaseعبدالسلام الأسمرNo ratings yet
- CV Dr. M. Yulianto Listiawan., DR., SPKK (K) Finsdv, FaadvDocument11 pagesCV Dr. M. Yulianto Listiawan., DR., SPKK (K) Finsdv, FaadvKharmijyNo ratings yet
- Pathophysiology ImpetigoDocument3 pagesPathophysiology ImpetigoAnne de VeraNo ratings yet
- Non Follicular PyodermaDocument1 pageNon Follicular PyodermaMagNo ratings yet
- Kode Diagnosa ICD PcareDocument5 pagesKode Diagnosa ICD Pcareheru suhartoNo ratings yet
- DermatologyDocument4 pagesDermatologyRemelou Garchitorena AlfelorNo ratings yet
- Mastery Question MDFDocument66 pagesMastery Question MDFshaaish100% (1)
- Topical Antibiotics For Skin InfectionsDocument4 pagesTopical Antibiotics For Skin InfectionsniklukNo ratings yet
- Pioderma - Viral Inf 2014Document132 pagesPioderma - Viral Inf 2014nanathursinaNo ratings yet
- Dermatology NotesDocument59 pagesDermatology NotesAbdullah Matar Badran50% (2)
- Impetigo FactsheetDocument2 pagesImpetigo FactsheetReza PahleviNo ratings yet
- ImpetigoDocument3 pagesImpetigoLynṅNo ratings yet
- 3) Bacterial Skin Infections Semi NotesDocument2 pages3) Bacterial Skin Infections Semi NotesIssa MoodNo ratings yet
- Infectous DiseaseDocument9 pagesInfectous DiseasejamikawasNo ratings yet
- 17 PDFDocument8 pages17 PDFHalfianiNo ratings yet
- Skin ConditionsDocument43 pagesSkin ConditionspdladvaNo ratings yet
- Cellulitis & Skin InfectionsDocument6 pagesCellulitis & Skin InfectionsPutriIffahNo ratings yet
- Cellulitis FactsDocument3 pagesCellulitis FactsCyril D. SuazoNo ratings yet
- 1) Bacterial Skin InfDocument32 pages1) Bacterial Skin InfsmrutuNo ratings yet
- Derma Notes 22pages. DR - Vishwa Medical CoachingDocument23 pagesDerma Notes 22pages. DR - Vishwa Medical CoachingΝίκος ΣυρίγοςNo ratings yet