You might also like
- Central Venous PressureDocument8 pagesCentral Venous PressureJen GarzoNo ratings yet
- Central Venous Preasure: By: Engkus Kusnadi, S.Kep., M.KesDocument22 pagesCentral Venous Preasure: By: Engkus Kusnadi, S.Kep., M.KesNenazNaziahNo ratings yet
- Central Venous Preasure: By: Engkus Kusnadi, S.Kep., M.KesDocument26 pagesCentral Venous Preasure: By: Engkus Kusnadi, S.Kep., M.KesShofarie AhmadNo ratings yet
- Central Venous PreasureDocument22 pagesCentral Venous PreasureD ZamiatNo ratings yet
- Sub - Medical Surgical Nursing: Assignment On CVP MonitoringDocument11 pagesSub - Medical Surgical Nursing: Assignment On CVP Monitoringkamini ChoudharyNo ratings yet
- Central Lines AND Arterial LinesDocument41 pagesCentral Lines AND Arterial LinesSalinKaurNo ratings yet
- CVP LineDocument26 pagesCVP LineÂbdàlláh Âl Ñàjjár0% (1)
- Central Venous Pressure (CVP)Document38 pagesCentral Venous Pressure (CVP)Kimberly Abella CabreraNo ratings yet
- kh7 CVPDocument50 pageskh7 CVPأبوأحمد الحكيمNo ratings yet
- CVPDocument23 pagesCVPShalini KaluraNo ratings yet
- Measuring Central Venous Pressure: Elaine ColeDocument8 pagesMeasuring Central Venous Pressure: Elaine ColednllkzaNo ratings yet
- CVPDocument25 pagesCVPNikhil YadavNo ratings yet
- Peripherally Inserted Central CatheterDocument4 pagesPeripherally Inserted Central CatheterDivine Grace Arreglo AbingNo ratings yet
- (FEU) Central Venous Pressure Notes PDFDocument25 pages(FEU) Central Venous Pressure Notes PDFBryJos tiongsonNo ratings yet
- CVP Final 2021Document11 pagesCVP Final 2021Ahmed AshrafNo ratings yet
- CVP PPPDocument13 pagesCVP PPPYep Yep100% (1)
- Christian Ian A DialysisDocument4 pagesChristian Ian A DialysisMc LagulaNo ratings yet
- Cateter Venoso Central PDFDocument37 pagesCateter Venoso Central PDFClaris PachecoNo ratings yet
- Central Venous PressureDocument22 pagesCentral Venous Pressurejhong100% (1)
- Seminar On Hemodynamic Monitoring: BY UMA Iind Year MSC NursingDocument52 pagesSeminar On Hemodynamic Monitoring: BY UMA Iind Year MSC NursingAyen AlingNo ratings yet
- CVP MonitoringDocument10 pagesCVP MonitoringRaghu RajanNo ratings yet
- 3730 Monitoring Hemodinamik-2019Document52 pages3730 Monitoring Hemodinamik-2019ojika olandaNo ratings yet
- CVP Care (Swapnil (Document18 pagesCVP Care (Swapnil (SWAPNIL WANJARINo ratings yet
- Take5 Hemodynamic1Document2 pagesTake5 Hemodynamic1est03No ratings yet
- CVP ReportDocument37 pagesCVP ReportJulienne Sanchez-SalazarNo ratings yet
- Essential Nursing Procedures Assignment - 092039Document14 pagesEssential Nursing Procedures Assignment - 092039IRA MONIQUE CABADENNo ratings yet
- Hemodynamics MonitoringDocument12 pagesHemodynamics MonitoringBhawna Joshi100% (3)
- CVP and Total Parenteral NutritionDocument4 pagesCVP and Total Parenteral Nutritionkenjam89mbNo ratings yet
- Avoiding Common Errors in The EdDocument18 pagesAvoiding Common Errors in The EdHandrian RahmanNo ratings yet
- Hemodynamic MonitoringDocument10 pagesHemodynamic MonitoringDivya Joy100% (1)
- Monitoring Hemodynamic StatusDocument50 pagesMonitoring Hemodynamic StatusShafiq Ur RahmanNo ratings yet
- Central Venous Pressure Monitoring ManualDocument6 pagesCentral Venous Pressure Monitoring ManualCristina L. JaysonNo ratings yet
- Central Venous PressureDocument39 pagesCentral Venous PressureJelly Rose Bajao Otayde100% (2)
- 106 Prefi Critical Care Nclex ReviewDocument10 pages106 Prefi Critical Care Nclex ReviewraigeneNo ratings yet
- Basic Intravenous TherapyDocument5 pagesBasic Intravenous TherapyJai Vee100% (1)
- Hemodynamic MonitoringDocument39 pagesHemodynamic MonitoringNor Jeannah PolaoNo ratings yet
- Central Venous CathetersDocument12 pagesCentral Venous CathetersarisastraNo ratings yet
- Arterial Lines MonitoringDocument13 pagesArterial Lines MonitoringJoseph Beredo33% (3)
- Pulmonary Artery Catheterization and MonitoringDocument31 pagesPulmonary Artery Catheterization and MonitoringVhince Norben PiscoNo ratings yet
- Chest Drainage Medical ManagementDocument3 pagesChest Drainage Medical ManagementPaul John RutaquioNo ratings yet
- CVP MonitoringDocument24 pagesCVP MonitoringChoji Heiwajima100% (1)
- WEEK-6 - Pulmonary Capillary Wedge PressureDocument5 pagesWEEK-6 - Pulmonary Capillary Wedge PressureYousuf Azhar Alamia0% (1)
- Meds-Study GuideDocument3 pagesMeds-Study Guidejackli21No ratings yet
- Flashcard Critical CareDocument11 pagesFlashcard Critical CaresnehaNo ratings yet
- Inferior Vena Cava Diameter and Collapsibility IndexDocument9 pagesInferior Vena Cava Diameter and Collapsibility IndexmalisalukmanNo ratings yet
- CVP MonitoringDocument64 pagesCVP MonitoringNárēsh Yadav GäddēNo ratings yet
- IV Therapy SsDocument56 pagesIV Therapy Sssaeed_chohan100% (8)
- Central Venous Access: RSUD Duren SawitDocument48 pagesCentral Venous Access: RSUD Duren SawitMonica HerdiatiNo ratings yet
- Activtiy UntitledDocument6 pagesActivtiy UntitledJan Cyrel ColomaNo ratings yet
- Management of The EVDDocument7 pagesManagement of The EVDplethoraldork100% (1)
- 2 150507152224 Lva1 App6892Document55 pages2 150507152224 Lva1 App6892poojaNo ratings yet
- DialysisDocument20 pagesDialysisSiwani rai100% (1)
- Sister Nivedita Govt. Nursing College Igmc, ShimlaDocument10 pagesSister Nivedita Govt. Nursing College Igmc, ShimlashivaniNo ratings yet
- Care of CVP LineDocument36 pagesCare of CVP LineArchana GaonkarNo ratings yet
- Central Venous Pressure MeasurementDocument6 pagesCentral Venous Pressure MeasurementghalaalsolumiNo ratings yet
- Atlas of 3D Transesophageal Echocardiography in Structural Heart Disease Interventions: Cases and VideosFrom EverandAtlas of 3D Transesophageal Echocardiography in Structural Heart Disease Interventions: Cases and VideosNo ratings yet
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- Mock Exam 51-100Document11 pagesMock Exam 51-100mike_steven12No ratings yet
- Mock ExamDocument26 pagesMock Exammike_steven12No ratings yet
- Mock Exam 101-150Document9 pagesMock Exam 101-150mike_steven120% (1)
- Mock Exam 1-50Document7 pagesMock Exam 1-50mike_steven12No ratings yet
- Information Sheet: Holy Family Parish Ministry of Altar ServersDocument2 pagesInformation Sheet: Holy Family Parish Ministry of Altar Serversmike_steven12No ratings yet
- Vital Sign Notes: Heart RateDocument2 pagesVital Sign Notes: Heart Ratemike_steven12No ratings yet
- Info GraphicDocument1 pageInfo Graphicmike_steven12No ratings yet
- Lab Values and Vital Signs PDFDocument4 pagesLab Values and Vital Signs PDFmike_steven12No ratings yet
- The Way - Our LadyDocument4 pagesThe Way - Our Ladymike_steven12No ratings yet
- Vital Sign Notes: Heart RateDocument2 pagesVital Sign Notes: Heart Ratemike_steven12No ratings yet
- GenChrist ChordsDocument8 pagesGenChrist Chordsmike_steven12No ratings yet
- Vital Sign Notes: Heart RateDocument2 pagesVital Sign Notes: Heart Ratemike_steven12No ratings yet
- Vital Sign Notes: Heart RateDocument2 pagesVital Sign Notes: Heart Ratemike_steven12No ratings yet
- 2015 BibleQuiz ReviewerDocument45 pages2015 BibleQuiz Reviewermike_steven1286% (7)
- SingDocument4 pagesSingmike_steven12No ratings yet
- SYLLABUS (Profession of Faith)Document1 pageSYLLABUS (Profession of Faith)mike_steven12No ratings yet
- CCA Information SheetDocument6 pagesCCA Information Sheetmike_steven12No ratings yet
- No One Like YouDocument1 pageNo One Like Youmike_steven12No ratings yet
- Morning OfferingDocument2 pagesMorning Offeringmike_steven12No ratings yet
- Prayer After Service at The Holy MassDocument1 pagePrayer After Service at The Holy Massmike_steven12No ratings yet
- Prayer Before Service at The Holy MassDocument1 pagePrayer Before Service at The Holy Massmike_steven12No ratings yet
- CATECHISM OUTLINE (YouCat)Document1 pageCATECHISM OUTLINE (YouCat)mike_steven12No ratings yet
- Blessed Be That Monotony of Hail MarysDocument2 pagesBlessed Be That Monotony of Hail Marysmike_steven12No ratings yet
- Friends of GodDocument1 pageFriends of Godmike_steven12No ratings yet
- NatscieDocument8 pagesNatsciemike_steven12No ratings yet
- Morning OfferingDocument2 pagesMorning Offeringmike_steven12No ratings yet
- Prayer Before Service at The Holy Mass - For ApprovalDocument1 pagePrayer Before Service at The Holy Mass - For Approvalmike_steven12No ratings yet
- No One Like YouDocument1 pageNo One Like Youmike_steven12No ratings yet
- Friends of GodDocument1 pageFriends of Godmike_steven12No ratings yet
- Catechism Outline (Youcat)Document1 pageCatechism Outline (Youcat)mike_steven12No ratings yet
- Toxicology CasesDocument65 pagesToxicology CasesLalo LandaNo ratings yet
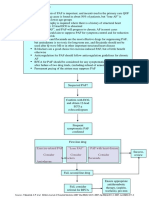
- Pathway DIAGNOSIS OF PAF FTRDocument1 pagePathway DIAGNOSIS OF PAF FTRYoan Eka Putra PalilingNo ratings yet
- 15 - CCLS - PharmacologyDocument32 pages15 - CCLS - PharmacologyVENKATESH RAMSALINo ratings yet
- Drug Study CARDIODocument17 pagesDrug Study CARDIODiannetotz Morales100% (1)
- Cardioversion of Atrial Fibrillation and AtrialDocument13 pagesCardioversion of Atrial Fibrillation and AtrialLabontu IustinaNo ratings yet
- Cardio QuestionsDocument21 pagesCardio QuestionsJenna AbuanNo ratings yet
- K - 7 Atrial Flutter (IKA)Document8 pagesK - 7 Atrial Flutter (IKA)thomasfelixNo ratings yet
- Short Answer Questions in AnaesthesiaDocument134 pagesShort Answer Questions in AnaesthesiaGlen Item92% (13)
- 04 Cardiotonic, AntharrythmicDocument125 pages04 Cardiotonic, Antharrythmic2nnfpjy5yvNo ratings yet
- EKG RhythmsDocument10 pagesEKG RhythmsQueenNo ratings yet
- Pharm Exam1Document17 pagesPharm Exam1Jill Putman Beistline75% (4)
- Full Download Book Usmle Step 2 Secrets PDFDocument41 pagesFull Download Book Usmle Step 2 Secrets PDFpeter.davis552100% (14)
- Current Clinical Strategies: Handbook of AnesthesiologyDocument180 pagesCurrent Clinical Strategies: Handbook of AnesthesiologydramaganaNo ratings yet
- Drug StudyDocument21 pagesDrug StudytyaneoNo ratings yet
- Serrano-Martin Et. Al. 2009b AMIO-MILTEDocument6 pagesSerrano-Martin Et. Al. 2009b AMIO-MILTEYael GarciaNo ratings yet
- Medication CardsDocument65 pagesMedication CardsMovaliya Ghanshyam80% (5)
- Managing Atrial Fibrillation in Patients With Heart Failure and Reduced Ejection FractionDocument18 pagesManaging Atrial Fibrillation in Patients With Heart Failure and Reduced Ejection FractionIsaac Martinez ArevaloNo ratings yet
- 2020 Canadian Cardiovascular SocietyCanadian Heart Rhythm Society Position Statement On The Management of Ventricular Tachycardia and Fibrillation in Patients With Structural Heart Disease PDFDocument15 pages2020 Canadian Cardiovascular SocietyCanadian Heart Rhythm Society Position Statement On The Management of Ventricular Tachycardia and Fibrillation in Patients With Structural Heart Disease PDFDiego MerchánNo ratings yet
- On Emergency DrugsDocument25 pagesOn Emergency DrugsBikram Chhetry100% (1)
- Dược Động Học SlideDocument24 pagesDược Động Học SlideDược NamNo ratings yet
- Guaranteed To Pass: Exam Tidbits in Easy To Digest, Bite Sized MorselsDocument2 pagesGuaranteed To Pass: Exam Tidbits in Easy To Digest, Bite Sized MorselsAmberNo ratings yet
- Drugs Used in Critica Care SettingDocument54 pagesDrugs Used in Critica Care SettingChandan KumarNo ratings yet
- "Emergency Drugs": Pictures/ Generic Name Brand Name/ Classification/ Stock Dose/ Indication Nursing ResponsibilitiesDocument7 pages"Emergency Drugs": Pictures/ Generic Name Brand Name/ Classification/ Stock Dose/ Indication Nursing ResponsibilitiesJohn Balgoa100% (2)
- Pepsci RecallDocument3 pagesPepsci RecallRumana AliNo ratings yet
- ACLS Post TestDocument6 pagesACLS Post TestSheila Tolentino-Belanio73% (77)
- Standardised Drug Infusion ConcentrationsDocument16 pagesStandardised Drug Infusion Concentrationsnot here 2make friends sorryNo ratings yet
- Case Study NCM 118Document14 pagesCase Study NCM 118Romzy BasañesNo ratings yet
- Drug Study AMIODARONE & PROPOFOLDocument3 pagesDrug Study AMIODARONE & PROPOFOLNIKKI CARYL ZAFRANo ratings yet
- Current News in CardiologyDocument428 pagesCurrent News in CardiologyDenisa DiaconuNo ratings yet
- 2019 Practice of Anesthesia For Infants and ChildrenDocument2 pages2019 Practice of Anesthesia For Infants and ChildrenJavier GlezqNo ratings yet