You might also like
- Massage Client Waiver Form 1 2Document1 pageMassage Client Waiver Form 1 2api-516845106No ratings yet
- Intake FormDocument1 pageIntake Formapi-358259684No ratings yet
- Client Info FormDocument2 pagesClient Info FormkamalsalmanNo ratings yet
- MassageTherapy IntakeFormDocument2 pagesMassageTherapy IntakeFormslbecker01No ratings yet
- Client Intake Form - Massage TherapyDocument3 pagesClient Intake Form - Massage TherapyRick TarletonNo ratings yet
- Client Intake Form - Therapeutic MassageDocument2 pagesClient Intake Form - Therapeutic MassagePeter SosaNo ratings yet
- Relax and Rejuvenate with Massage TypesDocument21 pagesRelax and Rejuvenate with Massage TypesArt Robin NagpacanNo ratings yet
- BROCHURE - Massage Therapy Final BrochureDocument2 pagesBROCHURE - Massage Therapy Final Brochurerlczech0348No ratings yet
- Bootcamp Registration Form-8Document4 pagesBootcamp Registration Form-8api-94490829No ratings yet
- Massage Therapy: Hotel Management SPHM HospitalityDocument23 pagesMassage Therapy: Hotel Management SPHM HospitalitySPHM Hospitality100% (2)
- Structured Touch MassageDocument5 pagesStructured Touch Massagegfrankel72No ratings yet
- Ef310 - Unit 8 Assignment PDFDocument4 pagesEf310 - Unit 8 Assignment PDFapi-533353748No ratings yet
- Daily Docket: Today'S Most Important ThingsDocument2 pagesDaily Docket: Today'S Most Important ThingsMatthew LevineNo ratings yet
- Best Body Massage Center - Full Body - Female To Male Parlour - Near BangaloreDocument12 pagesBest Body Massage Center - Full Body - Female To Male Parlour - Near BangalorePick my spaNo ratings yet
- Indian Head MassageDocument49 pagesIndian Head MassagekoekemoerNo ratings yet
- Massage Therapy Client Intake FormDocument4 pagesMassage Therapy Client Intake FormEverly Oballo100% (1)
- Sinus Massage By: Sushumna Mahesh What Is Sinus Pain?Document5 pagesSinus Massage By: Sushumna Mahesh What Is Sinus Pain?Julenda NikijuluwNo ratings yet
- I Am Fitness AgreementDocument1 pageI Am Fitness AgreementiamfitnessNo ratings yet
- Postnatal Class Enrollment Form SEODocument3 pagesPostnatal Class Enrollment Form SEOMihaelaNo ratings yet
- Massage Therapy EffectsDocument12 pagesMassage Therapy EffectsEkalevi FahlepieNo ratings yet
- New Member Intake Form: Personal InformationDocument3 pagesNew Member Intake Form: Personal InformationRui CunhaNo ratings yet
- Hygeia Lifestyle Intake QuestionnaireDocument6 pagesHygeia Lifestyle Intake QuestionnaireVivek GuptaNo ratings yet
- Patient Information and Benefits Assignment & ReleaseDocument17 pagesPatient Information and Benefits Assignment & ReleaseMr. Alma Myers, LAcNo ratings yet
- Pre-participation Physical Evaluation HISTORY and PHYSICAL EXAM FormsDocument2 pagesPre-participation Physical Evaluation HISTORY and PHYSICAL EXAM FormsCindy Hayes ShultzNo ratings yet
- S. Cole HW499 Unit 5 Power Point Massage TherapyDocument9 pagesS. Cole HW499 Unit 5 Power Point Massage TherapySifon ColeNo ratings yet
- The Virtual Yoga Teacher: ChallengeDocument19 pagesThe Virtual Yoga Teacher: ChallengeDivyaChettyNo ratings yet
- Massage Therapy - Workplace Massage - Chair Massage - Stress Management - Stress - Relaxation - Massage - T PDFDocument1 pageMassage Therapy - Workplace Massage - Chair Massage - Stress Management - Stress - Relaxation - Massage - T PDFnaveenNo ratings yet
- Clearance For Safe Exercise Participation: I. Health HistoryDocument3 pagesClearance For Safe Exercise Participation: I. Health HistoryejjohnsoNo ratings yet
- Healthform PDFDocument4 pagesHealthform PDFAdobo ManNo ratings yet
- MASSAGE EVIDENCE REVIEWDocument7 pagesMASSAGE EVIDENCE REVIEWRashoode Al-mezieneNo ratings yet
- Business & Insurance Info: PresentsDocument17 pagesBusiness & Insurance Info: PresentsАлексNo ratings yet
- DH Health Assessment FormDocument3 pagesDH Health Assessment FormRayceNo ratings yet
- 26.09.2020 Blog 2 - Mesmerising Massage Therapy With Phoenix Massage and WellnessDocument2 pages26.09.2020 Blog 2 - Mesmerising Massage Therapy With Phoenix Massage and WellnessPhoenix MassageNo ratings yet
- Freatured Listing: Dedicated Spa Directory in IndiaDocument20 pagesFreatured Listing: Dedicated Spa Directory in IndiaSpa RoyalNo ratings yet
- Intake Form Ficha de InformacionDocument2 pagesIntake Form Ficha de Informacionmaria mariaNo ratings yet
- Client Intake FormDocument2 pagesClient Intake FormPeter Sosa100% (1)
- Massage Client Intake Form PDFDocument2 pagesMassage Client Intake Form PDFSheila LaingNo ratings yet
- New Health and HistoryDocument3 pagesNew Health and HistorymredubzNo ratings yet
- BMMT Health FormDocument1 pageBMMT Health Formapi-232122843No ratings yet
- Health Information PrintDocument2 pagesHealth Information PrintCarole ArmsNo ratings yet
- Massage Client Intake FormDocument4 pagesMassage Client Intake FormyourlifelineNo ratings yet
- Patient Registration Form: General Information (Please Print Neatly)Document5 pagesPatient Registration Form: General Information (Please Print Neatly)Dan ThomasNo ratings yet
- Excel Patient FormsDocument10 pagesExcel Patient FormsGrayson Carwile CampbellNo ratings yet
- MicroCurrent Consent Form 2Document2 pagesMicroCurrent Consent Form 2suniel8080No ratings yet
- Intake FormDocument4 pagesIntake Formapi-217218803No ratings yet
- Case Histroy Form by Dr. Jawahar ShahDocument21 pagesCase Histroy Form by Dr. Jawahar ShahShubhanshi BhasinNo ratings yet
- Patientintakeform 2 FillableDocument2 pagesPatientintakeform 2 Fillableapi-519806395No ratings yet
- Health Questionnaire Patient IDDocument2 pagesHealth Questionnaire Patient IDfredNo ratings yet
- Client medical history and treatment detailsDocument3 pagesClient medical history and treatment detailsMa. Thea Diane BillonesNo ratings yet
- Referral LetterDocument3 pagesReferral LetterMa. Thea Diane BillonesNo ratings yet
- Green Lotus Health History FormDocument3 pagesGreen Lotus Health History Formkendra DenoNo ratings yet
- Patient Registration Form 13Document4 pagesPatient Registration Form 13windawaty humolaNo ratings yet
- Aromatherapy Patient Intake Form-BlankDocument8 pagesAromatherapy Patient Intake Form-Blankapi-282993701100% (2)
- Client Intake Form MassageDocument1 pageClient Intake Form MassageCarla LebronNo ratings yet
- Hands On Healing: Client Intake FormDocument2 pagesHands On Healing: Client Intake FormHealing Heaven AustraliaNo ratings yet
- Health Statement FormDocument1 pageHealth Statement FormALT IkedaNo ratings yet
- Consent FormDocument2 pagesConsent FormYsabel MendrosNo ratings yet
- Reiki Consent FormDocument3 pagesReiki Consent FormHealing Heaven AustraliaNo ratings yet
- YogaDocument1 pageYogaapi-422808692No ratings yet
- Client InformationDocument1 pageClient Informationapi-197836702No ratings yet
- Playroom in A Hospital: Jessica G. Marcelo Garcia, Yeimi Rivera Gonzalez, Lourdes Moreno de La O, Irene Olvera GarciaDocument4 pagesPlayroom in A Hospital: Jessica G. Marcelo Garcia, Yeimi Rivera Gonzalez, Lourdes Moreno de La O, Irene Olvera GarciaSarahi GonzalezNo ratings yet
- Case Taking Acc Different AuthorsDocument13 pagesCase Taking Acc Different AuthorsHarsha Koppula100% (1)
- Acute Pain Nursing Care PlanDocument3 pagesAcute Pain Nursing Care PlanTipey Segismundo100% (1)
- Healy Professional DeviceDocument1 pageHealy Professional DeviceBramarish KadakuntlaNo ratings yet
- Accidents Fact SheetDocument1 pageAccidents Fact SheetmajikNo ratings yet
- Difficult Patient Encounters: Assessing Pediatric Residents' Communication Skills Training NeedsDocument19 pagesDifficult Patient Encounters: Assessing Pediatric Residents' Communication Skills Training NeedsJesse M. MassieNo ratings yet
- Investigatory Project On AnalgesicsDocument30 pagesInvestigatory Project On AnalgesicsAnurag Singh100% (1)
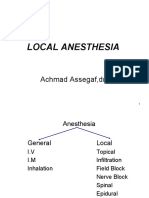
- Local Anesthesia: Achmad Assegaf, DR., SP - AnDocument48 pagesLocal Anesthesia: Achmad Assegaf, DR., SP - AnDesty ArianiNo ratings yet
- Revisi New Erni Juniartati Vol 08 No. 2Document8 pagesRevisi New Erni Juniartati Vol 08 No. 2Edi Pramana IINo ratings yet
- Pid OrthoDocument9 pagesPid OrthosapphireNo ratings yet
- 5.psychosocial Aspects of Health and DiseaseDocument30 pages5.psychosocial Aspects of Health and DiseaseFaisal MehboobNo ratings yet
- Pain Management and Unani MedicineDocument1 pagePain Management and Unani MedicineMSKCNo ratings yet
- Oet Writing Exercise AnswersDocument10 pagesOet Writing Exercise AnswersLia Angulo-Estrada95% (22)
- How To Write A SOAP Note-3-10Document2 pagesHow To Write A SOAP Note-3-10mohamed_musaferNo ratings yet
- Staged Approach For Rehabilitation ClassificationDocument10 pagesStaged Approach For Rehabilitation ClassificationCambriaChicoNo ratings yet
- LAENNEC Japan Bio Products Co., LTDDocument1 pageLAENNEC Japan Bio Products Co., LTDAnonymous UCc1qnmUnFNo ratings yet
- Blood Letting Therapy (Siravyadhana) in Acute Sciatica Pain (Gridhrasi)Document5 pagesBlood Letting Therapy (Siravyadhana) in Acute Sciatica Pain (Gridhrasi)YADU GOPANNo ratings yet
- 7 Steps HealDocument17 pages7 Steps HealAnonymous JkJ4CGwf100% (1)
- Psychiartry NotesDocument38 pagesPsychiartry NotesAlthea Lujille PinazoNo ratings yet
- Durere YoumansDocument171 pagesDurere YoumansIonut OlteanuNo ratings yet
- ASIA Impairment ScaleDocument10 pagesASIA Impairment Scaleazimahzainal211No ratings yet
- NCP For MyomectomyDocument3 pagesNCP For Myomectomyyasira100% (2)
- Hot Stone Massage BenefitsjhxnjDocument2 pagesHot Stone Massage Benefitsjhxnjsecondstove31No ratings yet
- Resident Fall and InjuryDocument5 pagesResident Fall and InjuryDebbie Cox MatthewsNo ratings yet
- Case Study QuestionnaireDocument6 pagesCase Study QuestionnaireKim TangoNo ratings yet
- Pediatrics Nursing L5Document89 pagesPediatrics Nursing L5MaxNo ratings yet
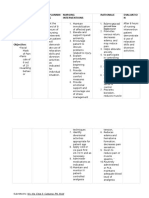
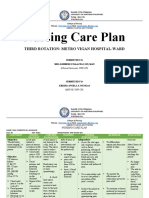
- Nursing Care Plan: Third Rotation: Metro Vigan Hospital-WardDocument5 pagesNursing Care Plan: Third Rotation: Metro Vigan Hospital-WardKrizha Angela NicolasNo ratings yet
- Case History FibromyalgiaDocument23 pagesCase History FibromyalgiaRAGUPATHYNo ratings yet
- ... My Reflection On Action (Leadershinp and Management)Document15 pages... My Reflection On Action (Leadershinp and Management)Yasmeen zulfiqarNo ratings yet
- Focus On Diagnosis of Acute Compartment Syndrome PDFDocument8 pagesFocus On Diagnosis of Acute Compartment Syndrome PDFMuthia DewiNo ratings yet