You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Pharmacology of Inotropes and VasopressorsDocument51 pagesPharmacology of Inotropes and VasopressorsApen Silaban100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Primary Trauma Care: Authors Douglas A Wilkinson and Marcus W SkinnerDocument51 pagesPrimary Trauma Care: Authors Douglas A Wilkinson and Marcus W SkinnerFahlevie EpinNo ratings yet
- Siu Yuen Surgery Notes PDFDocument213 pagesSiu Yuen Surgery Notes PDFAnonymous w4lLoMd7100% (1)
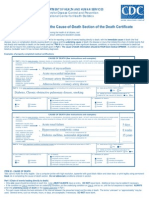
- Death CertificateDocument3 pagesDeath CertificateAllen Peter WeixlerNo ratings yet
- Haemodynamic MonitoringDocument128 pagesHaemodynamic MonitoringDr. KNo ratings yet
- Shock ExamDocument3 pagesShock ExamMilagros Fuertes Yosores100% (1)
- Emergency Nursing ExamDocument38 pagesEmergency Nursing Exammilayosores100% (4)
- PALS Provider Manual PDFDocument57 pagesPALS Provider Manual PDFtimie_reyes90% (21)
- QA Lesson Plan L3 First Aid at Work RQF - Including Catastrophic BleedingDocument41 pagesQA Lesson Plan L3 First Aid at Work RQF - Including Catastrophic BleedingPhysical Education Scotland88% (8)
- Sympathomimetic Drugs PharmacologyDocument10 pagesSympathomimetic Drugs PharmacologyHaroon JavedNo ratings yet
- Questions G 2Document8 pagesQuestions G 2Nader Smadi100% (1)
- Optimizing Fluid Therapy in Shock.10Document6 pagesOptimizing Fluid Therapy in Shock.10Paulo Victor100% (1)
- ICU-ED Clinical AssignmentDocument5 pagesICU-ED Clinical AssignmentMark LiebNo ratings yet
- Etica Medicala SeminarDocument18 pagesEtica Medicala SeminarFiosoiu Alexandru MirceaNo ratings yet
- Textbook ReadingDocument275 pagesTextbook ReadingNovitasari EkaNo ratings yet
- Hemodynamic MonitoringDocument4 pagesHemodynamic Monitoringgurneet kourNo ratings yet
- Geriatric Confusion CaseDocument8 pagesGeriatric Confusion CaseStarr NewmanNo ratings yet
- Journal Pediatric IndiaDocument5 pagesJournal Pediatric IndiaHhhNo ratings yet
- Approach To Septic ShockDocument16 pagesApproach To Septic ShockRaja EllysyaNo ratings yet
- Erdn NotesDocument10 pagesErdn NotesLucky GomezNo ratings yet
- DR Dhiman BanikCariogenic Shock Final 2022 DDDocument59 pagesDR Dhiman BanikCariogenic Shock Final 2022 DDCloudySkyNo ratings yet
- Classification of Injuries FMTDocument30 pagesClassification of Injuries FMTkhadzx100% (2)
- EGDTDocument33 pagesEGDTaLineLanNo ratings yet
- Abcde ApproachDocument3 pagesAbcde ApproachHala BahaaNo ratings yet
- Control Bleeding and ShockDocument6 pagesControl Bleeding and ShockElianeOliveiraNo ratings yet
- Pericardial Diseases: Acute PericarditisDocument26 pagesPericardial Diseases: Acute PericarditisamsirakNo ratings yet
- Blue FormDocument2 pagesBlue Formalin_capilnean8371No ratings yet
- 3rd - Neurogenic ShockDocument7 pages3rd - Neurogenic ShockjoidaNo ratings yet
- Perdarahan PeripartumDocument8 pagesPerdarahan PeripartumSuhatman AhNo ratings yet
- ABCDE. The Assessment of The Critically Ill PatientDocument4 pagesABCDE. The Assessment of The Critically Ill PatientGani mutiaraNo ratings yet