You might also like
- Portal Hypertension, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPortal Hypertension, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- RdsDocument25 pagesRdsEddogawa C' TaplakismeNo ratings yet
- Neonatal Exchange Transfusion GuideDocument9 pagesNeonatal Exchange Transfusion GuidedewpraNo ratings yet
- Congenital SyphilisDocument6 pagesCongenital SyphilisFrozen Pandora MahayaNo ratings yet
- Imuune Thrombocytopenia (Itp)Document34 pagesImuune Thrombocytopenia (Itp)Roshandiep GillNo ratings yet
- Idiopathic Thrombocytopenic PurpuraDocument10 pagesIdiopathic Thrombocytopenic PurpuramariakolandaNo ratings yet
- Perioperative Fluid Management in ChildrenDocument31 pagesPerioperative Fluid Management in ChildrenRashmi SahaNo ratings yet
- Liver Function Test FinalDocument98 pagesLiver Function Test FinalHussain AzharNo ratings yet
- Obstetrics Case PresentationDocument27 pagesObstetrics Case PresentationMahaprasad sahoo 77No ratings yet
- Physical Growth and Development: Different Aspects and AssessmentDocument60 pagesPhysical Growth and Development: Different Aspects and AssessmentDipti RamiNo ratings yet
- The West Bengal University of Health SciencesDocument9 pagesThe West Bengal University of Health Sciencesbhaskar rayNo ratings yet
- Neonatal Exchange Transfusion (Neonatal)Document8 pagesNeonatal Exchange Transfusion (Neonatal)Muhammad ShahbazNo ratings yet
- Chronic Otitis MediaDocument4 pagesChronic Otitis MediaOvyanda Eka MItraNo ratings yet
- RH IcompatibilityDocument3 pagesRH IcompatibilitySourabh SharafNo ratings yet
- Idiopathic Thrombocytopenic Purpura Case StudyDocument38 pagesIdiopathic Thrombocytopenic Purpura Case StudyKurbulNo ratings yet
- Idiopathic Thrombocytopenic PurpuraDocument8 pagesIdiopathic Thrombocytopenic PurpuraMonette Abalos MendovaNo ratings yet
- Chapter 14 - HematopathologyDocument66 pagesChapter 14 - Hematopathologynigel farageNo ratings yet
- Newborn Respiratory Distress 11.28.2011Document41 pagesNewborn Respiratory Distress 11.28.2011Emily EresumaNo ratings yet
- Hematology & Immune SystemDocument81 pagesHematology & Immune SystemAmanuel Maru100% (1)
- Submitted By: Diana M. Resultay A301/Group-3B Submitted To: Ms. ReyesDocument9 pagesSubmitted By: Diana M. Resultay A301/Group-3B Submitted To: Ms. ReyesDiannetotz MoralesNo ratings yet
- Medical Diseases Complicating Pregnancy: by The Name of AllahDocument45 pagesMedical Diseases Complicating Pregnancy: by The Name of Allah'محمد علي' محمد لافيNo ratings yet
- Hemolytic Disease of The NewbornDocument43 pagesHemolytic Disease of The Newbornalibayaty1No ratings yet
- Systemic Lupus Erythematosus (SLE)Document39 pagesSystemic Lupus Erythematosus (SLE)Nadya SabrinaNo ratings yet
- Acute Lymphoid LeukemiaDocument41 pagesAcute Lymphoid Leukemiaummi ulfahNo ratings yet
- Respiratory Distress Syndrome 1Document35 pagesRespiratory Distress Syndrome 1Marrah Avila AcuinNo ratings yet
- Sepsis Power Point Slide Presentation - The Guidelines - Implementation For The FutureDocument25 pagesSepsis Power Point Slide Presentation - The Guidelines - Implementation For The Futuremontie13No ratings yet
- Standard Treatment of Pyelonephritis in Pregnancy.4Document5 pagesStandard Treatment of Pyelonephritis in Pregnancy.4Maria Fe Esperanza MadambaNo ratings yet
- Ectopic PregnancyDocument76 pagesEctopic PregnancyVivian Jean TapayaNo ratings yet
- ABO IncompatibilityDocument2 pagesABO IncompatibilityeirikaesatcioNo ratings yet
- Anemia Anemia Describes The Condition in Which The Number of Red Blood Cells in The Blood Is Low. Probability & StatisticsDocument7 pagesAnemia Anemia Describes The Condition in Which The Number of Red Blood Cells in The Blood Is Low. Probability & StatisticsSahara GalayNo ratings yet
- Lecture Notes On AphDocument41 pagesLecture Notes On AphEyob MizanNo ratings yet
- Palliative Care for Cancer PatientsDocument39 pagesPalliative Care for Cancer PatientsBrodhing MotoVlogNo ratings yet
- Viral Hepatitis: Dr. Khaled JadallahDocument24 pagesViral Hepatitis: Dr. Khaled JadallahRashed ShatnawiNo ratings yet
- RH D Immunoglobulin (Anti-D)Document4 pagesRH D Immunoglobulin (Anti-D)Ywagar YwagarNo ratings yet
- NAFLD - NASH and Present & Future Management OptionsDocument78 pagesNAFLD - NASH and Present & Future Management OptionsSantosh AnandNo ratings yet
- PDF 075Document74 pagesPDF 075crystal_rc9No ratings yet
- Posterior Urethral ValveDocument6 pagesPosterior Urethral ValveMustafa AadanNo ratings yet
- Neonatal Jaundice: Causes and TreatmentsDocument18 pagesNeonatal Jaundice: Causes and TreatmentsArinaManaSikanaNo ratings yet
- Cirrhosis in Adults: Overview of Complications, General Management, and Prognosis - UpToDateDocument21 pagesCirrhosis in Adults: Overview of Complications, General Management, and Prognosis - UpToDateDan ChicinasNo ratings yet
- Neonatal InfectionsDocument19 pagesNeonatal InfectionsA B Siddique RiponNo ratings yet
- Pyloric Stenosis GuideDocument5 pagesPyloric Stenosis GuideMichael AlexanderNo ratings yet
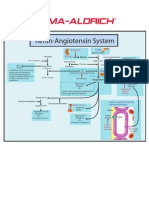
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- CPG Management of Neonatal Jaundice (Second Edition)Document62 pagesCPG Management of Neonatal Jaundice (Second Edition)umiraihana1100% (1)
- Fulminant Hepatic FailureDocument12 pagesFulminant Hepatic Failureafghansyah arfiantoNo ratings yet
- Malaria: Dr. Shree Narayan Yadav Internal Medicine Resident NamsDocument40 pagesMalaria: Dr. Shree Narayan Yadav Internal Medicine Resident Namsasyanadhikary18No ratings yet
- Malaria - MayoClinic PDFDocument6 pagesMalaria - MayoClinic PDFAdreiTheTripleANo ratings yet
- Central Venous PressureDocument10 pagesCentral Venous PressureAngelo ArquizaNo ratings yet
- Birth AsphyxiaDocument26 pagesBirth Asphyxiawizborrlyzo006No ratings yet
- Hereditary SpherocytosisDocument16 pagesHereditary Spherocytosisrizi2008No ratings yet
- Blood Administration: NRS 108 Essec County CollegeDocument22 pagesBlood Administration: NRS 108 Essec County CollegeDiah Puspita RiniNo ratings yet
- Development of The HeartDocument19 pagesDevelopment of The HeartYusuf UmarNo ratings yet
- Hyperemesis Gravidarum TreatmentDocument5 pagesHyperemesis Gravidarum TreatmentsalamredNo ratings yet
- Toxic Shock Syndrome - PPTX 1-1Document49 pagesToxic Shock Syndrome - PPTX 1-1Mohammed Khedr100% (1)
- Causes and Types of Rapidly Progressive GlomerulonephritisDocument28 pagesCauses and Types of Rapidly Progressive GlomerulonephritisPaul SinsNo ratings yet
- Spinal Cord InjuryDocument17 pagesSpinal Cord InjuryMuhammad FaridNo ratings yet
- Clinical Pediatric EvaluationDocument2 pagesClinical Pediatric EvaluationColeen VergaraNo ratings yet
- Kidney TransplantDocument3 pagesKidney TransplantSuneel Kumar PrajapatiNo ratings yet
- Von Willebrand DiseaseDocument9 pagesVon Willebrand DiseaserandyNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Swollen Kidney, (Hydronephrosis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSwollen Kidney, (Hydronephrosis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Valvular Heart Disease 2Document46 pagesValvular Heart Disease 2Topea BogdanNo ratings yet
- Echocardiographic Atlas of Adult Congenital Heart Disease: Hakimeh Sadeghian Zahra Savand-RoomiDocument486 pagesEchocardiographic Atlas of Adult Congenital Heart Disease: Hakimeh Sadeghian Zahra Savand-RoomiGeorgiana-Gratiela MalaescuNo ratings yet
- Case Report-Hemorragic Stroke-Fitra RulianDocument29 pagesCase Report-Hemorragic Stroke-Fitra RuliannabiyaNo ratings yet
- Lesson Plan On Myocardial InfarctionDocument4 pagesLesson Plan On Myocardial Infarctionpreet kaur0% (1)
- Functions of The Muscular System IncludeDocument8 pagesFunctions of The Muscular System IncludeDanesh CamachoNo ratings yet
- Ekg Plain and Simple 4th Edition Ellis Test BankDocument11 pagesEkg Plain and Simple 4th Edition Ellis Test Bankbrandicarrilloretfdampgw100% (10)
- Rasio Kadar Trigliserida-Kolesterol HDL Serum Tinggi Meningkatkan Keparahan Klinis Penderita Stroke Iskemik AkutDocument5 pagesRasio Kadar Trigliserida-Kolesterol HDL Serum Tinggi Meningkatkan Keparahan Klinis Penderita Stroke Iskemik AkutYasmeen BiandaNo ratings yet
- Cardiac Output MonitoringDocument17 pagesCardiac Output MonitoringRuchi VatwaniNo ratings yet
- Lymph and SpleenDocument4 pagesLymph and SpleenDaniel FischerNo ratings yet
- Midterm 3 Monitoring Heart RateDocument12 pagesMidterm 3 Monitoring Heart RateM. C. R.No ratings yet
- Paper C KMU 2019 cardiac mcqsDocument28 pagesPaper C KMU 2019 cardiac mcqsaizaz100% (1)
- Edema: Leyi Gu Renal Division, Renji HospitalDocument27 pagesEdema: Leyi Gu Renal Division, Renji HospitalIdham BaharudinNo ratings yet
- ACS Case BosDocument13 pagesACS Case BosChadi AzarNo ratings yet
- Levo-Milri 2021Document7 pagesLevo-Milri 2021Fer AlmazanNo ratings yet
- Cardiovascular Case StudiesDocument8 pagesCardiovascular Case StudiesLouise JohnsonNo ratings yet
- Disturbances of Blood CirculationDocument59 pagesDisturbances of Blood Circulationсветлый поповNo ratings yet
- Types and Characteristics of Vascular GraftsDocument27 pagesTypes and Characteristics of Vascular Graftso aburobNo ratings yet
- Concept Map Chap7 General Survey Vital SignsDocument1 pageConcept Map Chap7 General Survey Vital SignsEvelyn MoatsNo ratings yet
- Circulatory Disorders VocabDocument12 pagesCirculatory Disorders VocabMădălina Stănășel0% (1)
- Heart Murmurs ExplainedDocument7 pagesHeart Murmurs ExplainedOffvb MednuNo ratings yet
- Atlas of Vascular Surgery and Endovascular Therapy - Anatomy and Technique 1E 2014 PDF UnitedVRG 3 PDFDocument795 pagesAtlas of Vascular Surgery and Endovascular Therapy - Anatomy and Technique 1E 2014 PDF UnitedVRG 3 PDFOanaDavid100% (3)
- Cardiology NotesDocument13 pagesCardiology NotesFreeNursingNotes78% (9)
- 13) 07-07-2021 MD Faculty - Resi - Solve Class - Cardiology - Nephrology - Acute Medicine - 21 DR - Mazed 1 40Q SolveDocument6 pages13) 07-07-2021 MD Faculty - Resi - Solve Class - Cardiology - Nephrology - Acute Medicine - 21 DR - Mazed 1 40Q SolveashrafNo ratings yet
- Angina and MI Nursing Care ScenariosDocument3 pagesAngina and MI Nursing Care ScenariosMaye Arugay100% (1)
- Heart and Central VesselsDocument3 pagesHeart and Central VesselsSiege DiamondsNo ratings yet
- Cardiac Emergencies GuideDocument49 pagesCardiac Emergencies Guideraman kumari100% (3)
- Clinical Spectrum of Atherosclerotic Heart DiseaseDocument50 pagesClinical Spectrum of Atherosclerotic Heart Diseaseadamu mohammadNo ratings yet
- NCP PPHDocument2 pagesNCP PPHMark Joseph Christian100% (1)
- 2 Quarter 1 Module 2 CirculatoryDocument21 pages2 Quarter 1 Module 2 CirculatoryJasmine Paz0% (1)
- Congenital Heart Diseases: Charles University of Prague 2 Faculty of Medicine Filip KoubekDocument43 pagesCongenital Heart Diseases: Charles University of Prague 2 Faculty of Medicine Filip KoubekAdel HamzicNo ratings yet