You might also like
- 08 - Retrieving SQL Metadata and Improving SQL PerformanceDocument35 pages08 - Retrieving SQL Metadata and Improving SQL PerformanceChowdhury Golam KibriaNo ratings yet
- 07 - Programming With T-SQLDocument35 pages07 - Programming With T-SQLChowdhury Golam KibriaNo ratings yet
- 06 - Modifying Data in SQL ServerDocument27 pages06 - Modifying Data in SQL ServerChowdhury Golam KibriaNo ratings yet
- Curriculum Vitae of Chowdhury Golam Kibria: DependentsDocument12 pagesCurriculum Vitae of Chowdhury Golam Kibria: DependentsChowdhury Golam KibriaNo ratings yet
- Value Chain Case For Health Care ReformDocument4 pagesValue Chain Case For Health Care ReformChowdhury Golam KibriaNo ratings yet
- 05 - SET Operators Grouping and Windows FunctionsDocument30 pages05 - SET Operators Grouping and Windows FunctionsChowdhury Golam KibriaNo ratings yet
- 04 - Grouping and Aggregating DataDocument35 pages04 - Grouping and Aggregating DataChowdhury Golam KibriaNo ratings yet
- 01 - Introducing SQL Server 2012Document27 pages01 - Introducing SQL Server 2012Chowdhury Golam KibriaNo ratings yet
- 03 - SQL Server Data Types and FunctionsDocument37 pages03 - SQL Server Data Types and FunctionsChowdhury Golam KibriaNo ratings yet
- 02 - Advanced SELECT StatementsDocument36 pages02 - Advanced SELECT StatementsChowdhury Golam KibriaNo ratings yet
- Value Chain Vs Supply ChainDocument7 pagesValue Chain Vs Supply Chainsornapudi472No ratings yet
- Health Care As A Complex Adaptive SystemDocument10 pagesHealth Care As A Complex Adaptive SystemChowdhury Golam KibriaNo ratings yet
- Advertising and Promotion - Chapter 6Document39 pagesAdvertising and Promotion - Chapter 6Chowdhury Golam Kibria100% (1)
- The Information Value Chain Revisited - A Design School ModelDocument12 pagesThe Information Value Chain Revisited - A Design School ModelChowdhury Golam KibriaNo ratings yet
- The Knowledge Value ChainDocument14 pagesThe Knowledge Value ChainChowdhury Golam KibriaNo ratings yet
- Quinn 2000 Outsourcing InnovationDocument16 pagesQuinn 2000 Outsourcing Innovationlia_baikNo ratings yet
- The Knowledge Value ChainDocument14 pagesThe Knowledge Value ChainChowdhury Golam KibriaNo ratings yet
- Value Chain Case For Health Care ReformDocument4 pagesValue Chain Case For Health Care ReformChowdhury Golam KibriaNo ratings yet
- Six Sigma in Healthcare Value ChainDocument30 pagesSix Sigma in Healthcare Value ChainChowdhury Golam Kibria100% (2)
- Information Value ChainDocument47 pagesInformation Value ChainChowdhury Golam Kibria100% (1)
- Latent Variable in Business Logistics ResearchDocument29 pagesLatent Variable in Business Logistics ResearchChowdhury Golam KibriaNo ratings yet
- Health Care As A Complex Adaptive SystemDocument10 pagesHealth Care As A Complex Adaptive SystemChowdhury Golam KibriaNo ratings yet
- A Structural Equation Model of Supply Chain Management Strategies and Firm PerformanceDocument26 pagesA Structural Equation Model of Supply Chain Management Strategies and Firm PerformanceChowdhury Golam KibriaNo ratings yet
- Product Driven Supply ChainDocument15 pagesProduct Driven Supply ChainChowdhury Golam KibriaNo ratings yet
- Health Care Value ChainDocument24 pagesHealth Care Value ChainallisterotherNo ratings yet
- How Green Is The Supply ChainDocument40 pagesHow Green Is The Supply ChainChowdhury Golam KibriaNo ratings yet
- Value Chain Case For Health Care ReformDocument4 pagesValue Chain Case For Health Care ReformChowdhury Golam KibriaNo ratings yet
- Health Economic GuidelinesDocument79 pagesHealth Economic GuidelinesChowdhury Golam KibriaNo ratings yet
- Fixing The Health Care Supply ChainDocument4 pagesFixing The Health Care Supply ChainChowdhury Golam KibriaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Different Kinds of ObligationsDocument13 pagesDifferent Kinds of ObligationsDanica QuinacmanNo ratings yet
- Amway India Project ReportDocument30 pagesAmway India Project Reportcrtnngl086% (7)
- Gaelic FootballDocument2 pagesGaelic FootballcanelaconlecheNo ratings yet
- Logitech Case Analysis: Solving Problems of Transportation Cost and Political RiskDocument7 pagesLogitech Case Analysis: Solving Problems of Transportation Cost and Political RiskdinishaNo ratings yet
- Class 3-C Has A SecretttttDocument397 pagesClass 3-C Has A SecretttttTangaka boboNo ratings yet
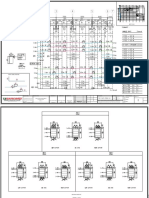
- Revised Y-Axis Beams PDFDocument28 pagesRevised Y-Axis Beams PDFPetreya UdtatNo ratings yet
- Rhetorical AnalysisDocument4 pagesRhetorical Analysisapi-495296714No ratings yet
- Narcotic Drugs (Control Enforcement and Sanctions) Law, 1990Document32 pagesNarcotic Drugs (Control Enforcement and Sanctions) Law, 1990Kofi Mc SharpNo ratings yet
- Hymns Vs Praise ChorusesDocument21 pagesHymns Vs Praise ChorusesLiem Sien LiongNo ratings yet
- Illustrative Bank Branch Audit FormatDocument4 pagesIllustrative Bank Branch Audit Formatnil sheNo ratings yet
- Inspirational Quotes ThesisDocument6 pagesInspirational Quotes Thesisanngarciamanchester100% (2)
- Stoddard v. USA - Document No. 2Document2 pagesStoddard v. USA - Document No. 2Justia.comNo ratings yet
- Pennycook Plagiarims PresentationDocument15 pagesPennycook Plagiarims Presentationtsara90No ratings yet
- ROCKS Air-to-Surface Missile Overcomes GPS Jamming in 38 CharactersDocument2 pagesROCKS Air-to-Surface Missile Overcomes GPS Jamming in 38 CharactersDaniel MadridNo ratings yet
- Electrical Energy Audit and SafetyDocument13 pagesElectrical Energy Audit and SafetyRam Kapur100% (1)
- Virgin Atlantic Strategic Management (The Branson Effect and Employee Positioning)Document23 pagesVirgin Atlantic Strategic Management (The Branson Effect and Employee Positioning)Enoch ObatundeNo ratings yet
- Boardingpass VijaysinghDocument2 pagesBoardingpass VijaysinghAshish ChauhanNo ratings yet
- B MBA I To IV Semesters Syllabus 2015-16Document258 pagesB MBA I To IV Semesters Syllabus 2015-16bcamaresh8054No ratings yet
- 2012 - Chapter 14 - Geberit Appendix Sanitary CatalogueDocument8 pages2012 - Chapter 14 - Geberit Appendix Sanitary CatalogueCatalin FrincuNo ratings yet
- CARPER LAD Form No. 25 Request For Cert - of RetentionDocument1 pageCARPER LAD Form No. 25 Request For Cert - of RetentionXaviera Marie100% (1)
- Exercise of Caution: Read The Text To Answer Questions 3 and 4Document3 pagesExercise of Caution: Read The Text To Answer Questions 3 and 4Shantie Susan WijayaNo ratings yet
- ThesisDocument310 pagesThesisricobana dimaraNo ratings yet
- 021810the History of Lent and EasterDocument28 pages021810the History of Lent and EasterTrinity of Orange100% (2)
- Green CHMDocument11 pagesGreen CHMShj OunNo ratings yet
- Economical Writing McCloskey Summaries 11-20Document4 pagesEconomical Writing McCloskey Summaries 11-20Elias Garcia100% (1)
- Soil Color ChartDocument13 pagesSoil Color ChartIqbal AamerNo ratings yet
- Ignorantia Juris Non ExcusatDocument3 pagesIgnorantia Juris Non ExcusatXymon Bassig0% (1)
- MS 1806 Inventory ModelDocument5 pagesMS 1806 Inventory ModelMariane MananganNo ratings yet
- English For Informatics EngineeringDocument32 pagesEnglish For Informatics EngineeringDiana Urian100% (1)
- Allotment Order 2022-23 - FIRST Round Arts - 52212302 - KARUNRAJ MDocument2 pagesAllotment Order 2022-23 - FIRST Round Arts - 52212302 - KARUNRAJ MKarun RajNo ratings yet