You might also like
- Newman's Billing and Coding Technicians Study GuideFrom EverandNewman's Billing and Coding Technicians Study GuideRating: 4.5 out of 5 stars4.5/5 (2)
- Production and Operations ManagementDocument284 pagesProduction and Operations Managementsnehal.deshmukh89% (28)
- Patient Information Sheet 091409Document2 pagesPatient Information Sheet 091409api-16816262No ratings yet
- The Feasibility of Establishing A Tax and Accounting Firm in Digos CityDocument2 pagesThe Feasibility of Establishing A Tax and Accounting Firm in Digos Citylorren4jeanNo ratings yet
- Luxus Hypermarket Service BlueprintDocument2 pagesLuxus Hypermarket Service BlueprintJITHA JOHNNY 22No ratings yet
- PCIDSSDocument13 pagesPCIDSSpriyanka_raut9021No ratings yet
- Citf Chapter 3-Ts StudentDocument14 pagesCitf Chapter 3-Ts StudentAlin RaissaNo ratings yet
- A Comparitive Study Between Amazon and Flipkarrt: MR - SandeepDocument64 pagesA Comparitive Study Between Amazon and Flipkarrt: MR - Sandeepj lohitha reddyNo ratings yet
- Performance Appraisal HR ProjectDocument92 pagesPerformance Appraisal HR Projectu4090230% (1)
- In-Patient Claim FormDocument2 pagesIn-Patient Claim Formfaisal_1241No ratings yet
- National Inurance Company Limited - Claim FormDocument3 pagesNational Inurance Company Limited - Claim FormfuckyouprettyNo ratings yet
- Claims Form For New India AssuranceDocument2 pagesClaims Form For New India AssuranceRafael BlackNo ratings yet
- UIICHdfc ClaimformDocument2 pagesUIICHdfc ClaimformdomyomglolNo ratings yet
- Claim Form NewDocument4 pagesClaim Form NewVicky GautamNo ratings yet
- NAIC Claim Form PDFDocument3 pagesNAIC Claim Form PDFMohit BaggaNo ratings yet
- Claim FormDocument3 pagesClaim FormSumit ManglaniNo ratings yet
- Claim FormDocument3 pagesClaim FormKhameer L Shah100% (1)
- Adamjee Insurance ClaimDocument2 pagesAdamjee Insurance ClaimubaidNo ratings yet
- 10 New India Assurance Company - Reimbursement Claim FormDocument3 pages10 New India Assurance Company - Reimbursement Claim FormbhurajeshNo ratings yet
- Head Office: 87, M G Road, Fort, Mumbai-400001: I. II - CLAIM NO.Document5 pagesHead Office: 87, M G Road, Fort, Mumbai-400001: I. II - CLAIM NO.gaddipati_ramuNo ratings yet
- Fixed Claim FormDocument2 pagesFixed Claim FormVikas GiriNo ratings yet
- GMC Claim Form How To File A ClaimDocument4 pagesGMC Claim Form How To File A ClaimtweetknotNo ratings yet
- OIC Claim FormDocument4 pagesOIC Claim FormPrashant SinghNo ratings yet
- Claim FormDocument5 pagesClaim Formsoumyadeep19478425No ratings yet
- Health Insurance Claim FormDocument3 pagesHealth Insurance Claim FormdivechahimanshuNo ratings yet
- Claim Form NewDocument4 pagesClaim Form Newparvazahmed03191No ratings yet
- Crewsure Claim Form (XLCatlin) 1.3Document2 pagesCrewsure Claim Form (XLCatlin) 1.3Andrei Belehuzi0% (1)
- National Insurance Company LimitedDocument4 pagesNational Insurance Company Limitedkaransandesara777No ratings yet
- FGH Claim Form - May 2014Document2 pagesFGH Claim Form - May 2014vijayNo ratings yet
- Claim Form: (For Reimbursement of Expenses)Document4 pagesClaim Form: (For Reimbursement of Expenses)Shankar NathNo ratings yet
- Health Total Claim FormDocument2 pagesHealth Total Claim Formpavan reddyNo ratings yet
- Mdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDocument5 pagesMdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormrhvenkatNo ratings yet
- f5192 PDFDocument2 pagesf5192 PDFVishal AggawalNo ratings yet
- HhhDocument4 pagesHhhMcnet WideNo ratings yet
- New India Assurance Hospitalisation Claim FormDocument3 pagesNew India Assurance Hospitalisation Claim Formharshmanu1612No ratings yet
- TPC Medical Claim FormDocument6 pagesTPC Medical Claim FormpenusilaNo ratings yet
- Job Loss Claim FormDocument3 pagesJob Loss Claim FormAbdulkhadarJilani ShaikNo ratings yet
- AB AROGYADAAN Group Medical InsuranceDocument6 pagesAB AROGYADAAN Group Medical Insuranceksantarao9700No ratings yet
- P.I. Client Demand PackageDocument6 pagesP.I. Client Demand PackageDrew BallNo ratings yet
- UIIC ClaimFormDocument2 pagesUIIC ClaimFormkarthikvel80No ratings yet
- Medical Claim Form (Reimbursement Only)Document2 pagesMedical Claim Form (Reimbursement Only)Muhammad Rizwan Tariq100% (1)
- InPatient Claim Form - Jubilee Life InsuranceDocument2 pagesInPatient Claim Form - Jubilee Life InsuranceAhmad Zubair40% (5)
- InPatient Claim Form - Jubilee Life InsuranceDocument2 pagesInPatient Claim Form - Jubilee Life InsuranceJawad MuhammadNo ratings yet
- OPD Form IHealthcare-2Document2 pagesOPD Form IHealthcare-2Masoom Kazmi100% (1)
- Pre Authorization Form IHealthcareDocument2 pagesPre Authorization Form IHealthcarecooljack08100% (1)
- Health Claim Intimation FormDocument3 pagesHealth Claim Intimation FormKiranmayi UppalaNo ratings yet
- Claimant Statement With ETF Mandate FormDocument6 pagesClaimant Statement With ETF Mandate FormKishan GarhtiyaNo ratings yet
- Claims reimbursement form submission guideDocument2 pagesClaims reimbursement form submission guideJoyce HerreraNo ratings yet
- Health Insurance product detailsDocument7 pagesHealth Insurance product detailssatishrasalNo ratings yet
- Mdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDocument4 pagesMdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDeepakNo ratings yet
- To, Shriram Life Insurance Company Limited.: Customer Mandate Cum Declaration Form For New BusinessDocument1 pageTo, Shriram Life Insurance Company Limited.: Customer Mandate Cum Declaration Form For New Businessdharam singhNo ratings yet
- 14) ELIB-Female CI-Claim FormDocument7 pages14) ELIB-Female CI-Claim Formbibianna93No ratings yet
- BCBSTX Halliburton Intl Claim FormDocument2 pagesBCBSTX Halliburton Intl Claim FormLoganBohannonNo ratings yet
- AXA Non Death Claim FormDocument4 pagesAXA Non Death Claim FormKenji ChinNo ratings yet
- Comforting Care ConsentsDocument14 pagesComforting Care ConsentsAmosNo ratings yet
- PH IcformDocument4 pagesPH IcformHihiNo ratings yet
- Adamjee Insurance medical claim formDocument2 pagesAdamjee Insurance medical claim formAmin RasheedNo ratings yet
- Easy Health Insurance Claim FormDocument3 pagesEasy Health Insurance Claim FormJanmejay SinghNo ratings yet
- Kolkata Claim Form - MD-IndiaDocument4 pagesKolkata Claim Form - MD-Indiadipankar0majumderNo ratings yet
- Claims Reimbursement Form GuideDocument2 pagesClaims Reimbursement Form Guideathenixia100% (1)
- CFPA-Medical ExpensesDocument2 pagesCFPA-Medical ExpensesDivya VoletiNo ratings yet
- Etiqa Out Patient Claim FormDocument1 pageEtiqa Out Patient Claim FormAlmecestrisNo ratings yet
- TEMPLATE Etiqa Out Patient Claim FormDocument1 pageTEMPLATE Etiqa Out Patient Claim FormEvoy EstradaNo ratings yet
- Claims Reimbursement Form: Member General InformationDocument1 pageClaims Reimbursement Form: Member General InformationFirmament DevelopmentNo ratings yet
- Maxicare Claims Reimbursement FormDocument2 pagesMaxicare Claims Reimbursement Formokong bokongNo ratings yet
- Womens Clothing Market Analysis Report - 2010Document24 pagesWomens Clothing Market Analysis Report - 2010u409023No ratings yet
- Small Scale Industries in IndiaDocument19 pagesSmall Scale Industries in Indiau409023No ratings yet
- Into Duct Ion To CBDocument19 pagesInto Duct Ion To CBishwar_ind2002No ratings yet
- Bhumi Putra Seva Pratisthana-UndertakingDocument3 pagesBhumi Putra Seva Pratisthana-Undertakingu409023No ratings yet
- Advertisement For Class III 16.05.2013Document11 pagesAdvertisement For Class III 16.05.2013ramu0923No ratings yet
- 79 BiologyDocument22 pages79 Biologyapi-238757880No ratings yet
- Siku Final Project-With Page NumberDocument86 pagesSiku Final Project-With Page Numberu409023No ratings yet
- Emami Paper Code of ConductDocument6 pagesEmami Paper Code of Conductu409023No ratings yet
- 79 BiologyDocument22 pages79 Biologyapi-238757880No ratings yet
- 5150 - Session 1 Operations Management Framework (B)Document5 pages5150 - Session 1 Operations Management Framework (B)u409023No ratings yet
- PHD App FormDocument4 pagesPHD App Formu409023No ratings yet
- Recog FormDocument8 pagesRecog Formu409023No ratings yet
- CRM Implementation Case Study in Construction SectorDocument10 pagesCRM Implementation Case Study in Construction Sectoru409023No ratings yet
- ICICI Bank Acquires Bank of Rajasthan For Rs 2,161 CroreDocument11 pagesICICI Bank Acquires Bank of Rajasthan For Rs 2,161 Croreu409023No ratings yet
- 5150 - Session 1 Operations Management Framework (B)Document5 pages5150 - Session 1 Operations Management Framework (B)u409023No ratings yet
- Hero Honda FinalDocument20 pagesHero Honda Finalu409023No ratings yet
- Franchise LatestDocument21 pagesFranchise Latestu409023No ratings yet
- 5150 - Session 1 Operations Management Framework (B)Document5 pages5150 - Session 1 Operations Management Framework (B)u409023No ratings yet
- Accounts Chapter-Wise Test 5 (Suggested Answers)Document7 pagesAccounts Chapter-Wise Test 5 (Suggested Answers)Shweta BhadauriaNo ratings yet
- Fixed DepositsDocument1 pageFixed DepositsTiso Blackstar GroupNo ratings yet
- Order ListDocument4 pagesOrder ListdienesurNo ratings yet
- GIVING DirectionsDocument1 pageGIVING DirectionsLita OktaviantariNo ratings yet
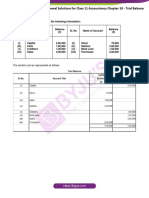
- Ts Grewal Solutions For Class 11 Accountancy Chapter 10 TrialDocument22 pagesTs Grewal Solutions For Class 11 Accountancy Chapter 10 TrialMantejNo ratings yet
- Performance Analysis of Modulation Schemes for 5G NetworksDocument52 pagesPerformance Analysis of Modulation Schemes for 5G Networksbelacheweshetu222No ratings yet
- Credit Appraisal For Working Capital and Term LoanDocument114 pagesCredit Appraisal For Working Capital and Term LoanAkanksha Kapoor100% (2)
- MKTG103 - ECOMMERCE AND DIGITAL MARKETINGDocument24 pagesMKTG103 - ECOMMERCE AND DIGITAL MARKETINGChona MarieNo ratings yet
- Label - 1663795065759 - 1 2Document1 pageLabel - 1663795065759 - 1 2Tazkhan123No ratings yet
- How Internet Works On Mobile DevicesDocument6 pagesHow Internet Works On Mobile DevicesBiruk BirhanuNo ratings yet
- 03102019112950pbnr06ed8wsuozgckh Estatement 092019 2202Document9 pages03102019112950pbnr06ed8wsuozgckh Estatement 092019 2202Manoj EmmidesettyNo ratings yet
- Fibocom FG360 EAU Datasheet - V1.7Document2 pagesFibocom FG360 EAU Datasheet - V1.7kashif bharwana TvNo ratings yet
- Chapter+4+ +Audit+of+Receivables+ (Part+1)Document10 pagesChapter+4+ +Audit+of+Receivables+ (Part+1)Dan MorettoNo ratings yet
- OpTransactionHistory09 06 2022Document4 pagesOpTransactionHistory09 06 2022vasant ugaleNo ratings yet
- Shawacademy Invoice Hr5518nRSAQFc0YeC PDFDocument1 pageShawacademy Invoice Hr5518nRSAQFc0YeC PDFAdrian Joseph NuñezNo ratings yet
- Glencoe Accounting Chp20Document26 pagesGlencoe Accounting Chp20Trisha Mae Bahande100% (2)
- Aviva - MINDEF - MHA - Group Term Life Product SummaryDocument4 pagesAviva - MINDEF - MHA - Group Term Life Product SummaryYew Kit QuekNo ratings yet
- Pharmaceutical Regulatory InspectionsDocument2 pagesPharmaceutical Regulatory InspectionsTim SandleNo ratings yet
- Unit 6Document19 pagesUnit 6ChandrakantBangarNo ratings yet
- International Roaming - Terms & ConditionsDocument1 pageInternational Roaming - Terms & ConditionsPatel KevalNo ratings yet
- Contents Property Loss InventoryDocument3 pagesContents Property Loss InventoryjanNo ratings yet
- PaperDocument4 pagesPaperamirNo ratings yet
- Test Cases MM Migo PostingDocument2 pagesTest Cases MM Migo Postingrodrigues_franc1565No ratings yet
- Park Bill 1Document2 pagesPark Bill 1sourabhNo ratings yet
- Conhecimento de Embarque.Document2 pagesConhecimento de Embarque.Aleandro Vasconcelos NascimentoNo ratings yet