You might also like
- Respiratory SystemDocument55 pagesRespiratory SystemEndla SriniNo ratings yet
- 8.respiration 2023Document12 pages8.respiration 2023Alina AtherNo ratings yet
- Pathophysiology of Chronic Obstructive Pulmonary DisorderDocument2 pagesPathophysiology of Chronic Obstructive Pulmonary DisorderBlessyl Mae EstenzoNo ratings yet
- PathophysiologyDocument1 pagePathophysiologyChua CandiceNo ratings yet
- Broncho 2Document4 pagesBroncho 2hotteenstar_23No ratings yet
- Culture and Sensitivity: InhalationDocument3 pagesCulture and Sensitivity: Inhalationjamie carpioNo ratings yet
- Modul 1Document28 pagesModul 1aszmadie81No ratings yet
- Med SurgDocument3 pagesMed SurgShaira Mae GordoraNo ratings yet
- Respiratory PhysiologyDocument42 pagesRespiratory PhysiologyvtnvmycdvgNo ratings yet
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaJeffrey Ramos100% (1)
- Anestesia Torax 2Document16 pagesAnestesia Torax 2Oscar Escobedo DamianNo ratings yet
- Predisposing Factors: Precipitating Factors: Contributing FactorsDocument6 pagesPredisposing Factors: Precipitating Factors: Contributing FactorsKen SimonNo ratings yet
- PEDIA-Emphysema and Atelectasis, Overinflation Diseases of The Pleura, Pleural Effusion, Tumors (Dr. Talatala)Document2 pagesPEDIA-Emphysema and Atelectasis, Overinflation Diseases of The Pleura, Pleural Effusion, Tumors (Dr. Talatala)Monique BorresNo ratings yet
- Oxygenation - 1Document7 pagesOxygenation - 1Cielo SanchezNo ratings yet
- Ineffective Airway Clearance Related To BronchospasmDocument2 pagesIneffective Airway Clearance Related To BronchospasmReylan Garcia100% (4)
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaJesselle LasernaNo ratings yet
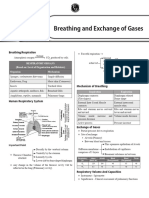
- 64d0d71d2a4c6c00193d7762 - ## - Breathing and Exchange of Gases Short NotesDocument2 pages64d0d71d2a4c6c00193d7762 - ## - Breathing and Exchange of Gases Short Notesjai maa Durga aadi parashaktiNo ratings yet
- To Maintain Patent Airway. (-: Surgical Nursing: Clinical Management For Positive Outcomes (Vol. 1)Document3 pagesTo Maintain Patent Airway. (-: Surgical Nursing: Clinical Management For Positive Outcomes (Vol. 1)Clint Delacruz50% (4)
- Lung Sounds TBL GuideDocument17 pagesLung Sounds TBL GuideJolaine ValloNo ratings yet
- Pa ThoDocument3 pagesPa Thotammy_deguzman5223No ratings yet
- Ncma113-Respiratory and Nursing CareDocument5 pagesNcma113-Respiratory and Nursing Careroldanmarygrace023No ratings yet
- Aljean Altheo L. Artillo BSN-3B 1. What Are The Pathophysiologies of Chronic Obstructive Pulmonary Disease (COPD) ?Document2 pagesAljean Altheo L. Artillo BSN-3B 1. What Are The Pathophysiologies of Chronic Obstructive Pulmonary Disease (COPD) ?Al TheóNo ratings yet
- 7.1 (LEC) - Functional Anatomy of Respiratory System and Mechanics of BreathingDocument9 pages7.1 (LEC) - Functional Anatomy of Respiratory System and Mechanics of BreathingKenneth TorresNo ratings yet
- Textbook Discussion On Acute Community-Acquired Pneumonia (BSN 3A-Group 6)Document9 pagesTextbook Discussion On Acute Community-Acquired Pneumonia (BSN 3A-Group 6)Jica Marie Bandiola GicaroNo ratings yet
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaJuneNo ratings yet
- 1 Breathing Mechanism 10Document2 pages1 Breathing Mechanism 10chinpy088464No ratings yet
- pg36-37 of Pneumothorax Case StudyDocument2 pagespg36-37 of Pneumothorax Case Studyikemas100% (1)
- (PULMO) - ABG Interpretation PDFDocument7 pages(PULMO) - ABG Interpretation PDFKeith LajotNo ratings yet
- Iv. Pathophysiology 1. Schematic Diagram Book Based Pathophysiology: Precipitating/Modifiable Factors Non Modifiable / Predisposing FactorsDocument2 pagesIv. Pathophysiology 1. Schematic Diagram Book Based Pathophysiology: Precipitating/Modifiable Factors Non Modifiable / Predisposing Factorsikemas67% (6)
- Nayli Bio SBP 2019 EseiDocument5 pagesNayli Bio SBP 2019 EseiEqis AlfiesyaNo ratings yet
- Respiratory SystemDocument340 pagesRespiratory SystemBHUWAN BASKOTANo ratings yet
- Sample ChapterDocument6 pagesSample ChapterSupaporn MarknuiNo ratings yet
- Covid NCPDocument6 pagesCovid NCPNathalia Cabalse100% (2)
- SARS PathophysioDocument2 pagesSARS PathophysioLouise BravoNo ratings yet
- Pneumocystis Pneumonia in an Elderly Heavy SmokerDocument2 pagesPneumocystis Pneumonia in an Elderly Heavy SmokerKismet SummonsNo ratings yet
- Managing Impaired Gas Exchange and Ineffective Airway ClearanceDocument27 pagesManaging Impaired Gas Exchange and Ineffective Airway ClearancecuakialyannaNo ratings yet
- Breathing and gas exchangeDocument10 pagesBreathing and gas exchangeramakant chobheNo ratings yet
- 2 Books 1. Notebooks 2. Exercises & ExperimentsDocument29 pages2 Books 1. Notebooks 2. Exercises & ExperimentsAi DaNo ratings yet
- Ineffective Airway ClearanceDocument6 pagesIneffective Airway ClearanceKarl Angelo MontanoNo ratings yet
- Pathophysiology EmphysemaDocument1 pagePathophysiology Emphysemanursing concept mapsNo ratings yet
- Respiratory System Mim Gozey PDFDocument80 pagesRespiratory System Mim Gozey PDFMim GozeyNo ratings yet
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaAzria John DemetriNo ratings yet
- Respi 2Document11 pagesRespi 2Jeno SigamaniNo ratings yet
- Finals Quiz 1 TransDocument14 pagesFinals Quiz 1 Transjade jaymeNo ratings yet
- Respiratory Physiology OverviewDocument7 pagesRespiratory Physiology OverviewMac Vince HipolitoNo ratings yet
- MEDSRUG Respiratory System NotesDocument6 pagesMEDSRUG Respiratory System NotesMichaela Katrice MacabangunNo ratings yet
- Chapter 20 OxygenationDocument31 pagesChapter 20 OxygenationHannah Lat VillavicencioNo ratings yet
- NCP MontanoDocument7 pagesNCP MontanoKarl Angelo MontanoNo ratings yet
- Upper Airway InfectionsDocument5 pagesUpper Airway InfectionsTreesa LouiseNo ratings yet
- Tugas Bu ReniDocument23 pagesTugas Bu Reniayu novita sariNo ratings yet
- Resp ExaminationDocument2 pagesResp ExaminationphreakyfilNo ratings yet
- Lower Respiratory System GlossaryDocument2 pagesLower Respiratory System GlossaryLarissa ShevchenkoNo ratings yet
- Acute Respiratory Failure Pa Tho PhysiologyDocument4 pagesAcute Respiratory Failure Pa Tho Physiologyroseanne18100% (4)
- Asthma and Emphysema Nursing CareDocument28 pagesAsthma and Emphysema Nursing CareSOPHIA PILLENANo ratings yet
- Pipes of the Church Organ - A Selection of Classic Articles on Organ Design and ConstructionFrom EverandPipes of the Church Organ - A Selection of Classic Articles on Organ Design and ConstructionNo ratings yet
- Anatomy of Voice: How to Enhance and Project Your Best VoiceFrom EverandAnatomy of Voice: How to Enhance and Project Your Best VoiceRating: 4 out of 5 stars4/5 (3)
- ARDS (Dr. Edi Nurtjahja - SP.P)Document23 pagesARDS (Dr. Edi Nurtjahja - SP.P)Mirna Ayu Permata SariNo ratings yet
- Protocol For Heart Rate Variability Biofeedback TrainingDocument13 pagesProtocol For Heart Rate Variability Biofeedback TrainingLevente BalázsNo ratings yet
- Nursing Management of Respiratory DisordersDocument151 pagesNursing Management of Respiratory DisordersAbirajan100% (2)
- The Safe and Simple Way To Set PEEP... and More !Document4 pagesThe Safe and Simple Way To Set PEEP... and More !ArNo ratings yet
- HydrotherapyDocument26 pagesHydrotherapyMohd Ismarezza100% (2)
- Soal 21Document4 pagesSoal 21obhetzNo ratings yet
- Plant and Animal Cell DifferencesDocument8 pagesPlant and Animal Cell DifferencesAnupam DasNo ratings yet
- Suctioning HandoutsDocument3 pagesSuctioning HandoutsErika ArceoNo ratings yet
- Occupational Lung DiseasesDocument3 pagesOccupational Lung DiseasesDjdjjd SiisusNo ratings yet
- Nursing Care of Child Respiratory DisordersDocument31 pagesNursing Care of Child Respiratory DisordersCnette S. LumboNo ratings yet
- Biological PsychologicalDocument4 pagesBiological Psychologicalfebria fadhilahNo ratings yet
- Vi. Nursing Care PlanDocument3 pagesVi. Nursing Care PlanJopaii TanakaNo ratings yet
- Anatomy of The Respiratory System - Dr. NdukuiDocument32 pagesAnatomy of The Respiratory System - Dr. Ndukuiglenian560No ratings yet
- Mechanical VentilationDocument18 pagesMechanical VentilationM BNo ratings yet
- Arterial Blood Gas AnalysisDocument8 pagesArterial Blood Gas AnalysisMichael NapoleonNo ratings yet
- Jurnal-Amphibi ReptilDocument12 pagesJurnal-Amphibi ReptilMohamad AfifudinNo ratings yet
- Biology 5090 12 Paper 1 Question Paper Mayjue 2013Document16 pagesBiology 5090 12 Paper 1 Question Paper Mayjue 2013Raja Muda Raja NgahNo ratings yet
- Artificial AirwaysDocument17 pagesArtificial AirwaysSri DarmayantiNo ratings yet
- 9781786321633Document125 pages9781786321633Leanna Sutherland-AliNo ratings yet
- Biology - Physics Chemistry MCQS: Gyanm'S General Awareness - November 2014Document13 pagesBiology - Physics Chemistry MCQS: Gyanm'S General Awareness - November 2014santosh.manojNo ratings yet
- MetrorrhagiaDocument24 pagesMetrorrhagiaMatt SarigumbaNo ratings yet
- Body Systems Module Complete (Highlighted Endocrine and Nervous)Document19 pagesBody Systems Module Complete (Highlighted Endocrine and Nervous)Ramon GasgasNo ratings yet
- Introduction To RespirationDocument14 pagesIntroduction To RespirationAzneezal Ar-RashidNo ratings yet
- Approch To StridorDocument27 pagesApproch To Stridoraltabeb hasoon67% (3)
- BREATHING EXERCISES GUIDEDocument32 pagesBREATHING EXERCISES GUIDEEvan Permana Putra100% (1)
- TonsilsDocument9 pagesTonsilstasnimNo ratings yet
- Pre Eclampsia ErDocument41 pagesPre Eclampsia ErKacelyn QuibanNo ratings yet
- Bi PAPDocument54 pagesBi PAPharshadNo ratings yet
- Science: Quarter 1 - Module 1Document10 pagesScience: Quarter 1 - Module 1RUTH PIANGNo ratings yet
- Laryngeal Obstruction: Narciso A. CañibanDocument54 pagesLaryngeal Obstruction: Narciso A. Cañibanalexandrajane200767% (3)