You might also like
- Executive Function and Self-Regulation in ChildrenFrom EverandExecutive Function and Self-Regulation in ChildrenRating: 5 out of 5 stars5/5 (2)
- Short Sensory ProfileDocument11 pagesShort Sensory ProfileNurul Izzah Wahidul Azam100% (1)
- Sensory Diet: Prepared by Christy E. Yee, OTRDocument12 pagesSensory Diet: Prepared by Christy E. Yee, OTRAlexandra StăncescuNo ratings yet
- Sensory Profile: Submitted By-Amandeep Kaur M.O.T-Neuro, Sem 3 ENROLLMENT NO - A138141620004 Guided by - Ruby Ma'AmDocument42 pagesSensory Profile: Submitted By-Amandeep Kaur M.O.T-Neuro, Sem 3 ENROLLMENT NO - A138141620004 Guided by - Ruby Ma'Amamandeep kaurNo ratings yet
- Sensory Diet Handout for Developmental FXDocument7 pagesSensory Diet Handout for Developmental FXpratibhaumrariya100% (1)
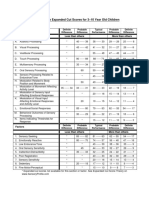
- Sensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenDocument1 pageSensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenAyra MagpiliNo ratings yet
- Supporting Children To Participate Successfully in Everyday Life Using Sensory Processing KnowledgeDocument19 pagesSupporting Children To Participate Successfully in Everyday Life Using Sensory Processing Knowledgeapi-26018051100% (1)
- Day 1: The Ultimate Guide To Decoding A Child's Sensory SystemDocument45 pagesDay 1: The Ultimate Guide To Decoding A Child's Sensory SystemLuca ServentiNo ratings yet
- The Assessment of Executive Functioning in ChildrenDocument37 pagesThe Assessment of Executive Functioning in Childrenluistxo2680No ratings yet
- Helping Hands-Website InformationDocument17 pagesHelping Hands-Website InformationDiana Moore Díaz100% (1)
- Using Sensory Integration andDocument9 pagesUsing Sensory Integration andVero MoldovanNo ratings yet
- Occupational Therapy Ia Sample ReportsDocument11 pagesOccupational Therapy Ia Sample Reportssneha duttaNo ratings yet
- 11 17 17 Treatment PlanDocument7 pages11 17 17 Treatment Planapi-435469413No ratings yet
- 132 Sensory Diet 090212Document2 pages132 Sensory Diet 090212Sally Vesper100% (1)
- Marcus Evaluation - StruthersDocument8 pagesMarcus Evaluation - Struthersapi-355500890No ratings yet
- A Review of Pediatric Assessment Tools For Sensory Integration AOTADocument3 pagesA Review of Pediatric Assessment Tools For Sensory Integration AOTAhelenzhang888No ratings yet
- Winnie Dunn Sensory Profile PDFDocument17 pagesWinnie Dunn Sensory Profile PDFYonaa K100% (1)
- Ota Watertown Si Clinical Assessment WorksheetDocument4 pagesOta Watertown Si Clinical Assessment WorksheetPaulinaNo ratings yet
- Supporting Therapy in The Classroom Strategies For OccupationalDocument70 pagesSupporting Therapy in The Classroom Strategies For Occupationalapi-451269263No ratings yet
- Ot GuidelinesDocument107 pagesOt GuidelinesAhmed MaherNo ratings yet
- Sensory Curriculum For Individuals On The Autism SpectrumDocument5 pagesSensory Curriculum For Individuals On The Autism SpectrumSuperfixen100% (1)
- 7 (SPM™) Sensory Processing Measure™ - WPSDocument1 page7 (SPM™) Sensory Processing Measure™ - WPSVINEET GAIROLA14% (7)
- Sensory Regulation ConferenceDocument19 pagesSensory Regulation ConferenceSebastian Pinto ReyesNo ratings yet
- Sensory Integration PDFDocument1 pageSensory Integration PDFmofasorgNo ratings yet
- Making Sense Sensory Processing Disorder103114Document61 pagesMaking Sense Sensory Processing Disorder103114Branislava Jaranovic Vujic100% (5)
- Sensory Integration in The Home: An OverviewDocument28 pagesSensory Integration in The Home: An OverviewEileen Grant100% (6)
- Motor Skills AutismDocument16 pagesMotor Skills AutismmarkonahNo ratings yet
- Sensory AssesmentDocument19 pagesSensory AssesmentBurçin KaynakNo ratings yet
- Beery Vmi Performance in Autism Spectrum DisorderDocument33 pagesBeery Vmi Performance in Autism Spectrum DisorderJayminertri Minorous100% (1)
- Sensory Processing 101: Understanding Sensory Challenges in ASDDocument75 pagesSensory Processing 101: Understanding Sensory Challenges in ASDjahirmiltonNo ratings yet
- Sensory Profile PowerpointDocument21 pagesSensory Profile PowerpointLama NammouraNo ratings yet
- Occupational Therapy - Play, SIs and BMTsDocument3 pagesOccupational Therapy - Play, SIs and BMTsAnnbe Barte100% (1)
- InTech-Sensory Motor Development in AutismDocument26 pagesInTech-Sensory Motor Development in AutismTânia DiasNo ratings yet
- Case StudyDocument12 pagesCase Study宗轶烜100% (1)
- Facilitation Techniques in Prone PositionDocument37 pagesFacilitation Techniques in Prone PositionMartha FrankNo ratings yet
- Sensory Assessment ChecklistDocument3 pagesSensory Assessment ChecklistElaime MaciquesNo ratings yet
- Screening SensorimotorDocument29 pagesScreening Sensorimotoramitesh_mpthNo ratings yet
- Sensory Processing Disorder Checklist: Signs of DysfunctionDocument7 pagesSensory Processing Disorder Checklist: Signs of DysfunctionLalitha Raja100% (1)
- Early Autism Red Flags Infants Toddlers PreschoolersDocument3 pagesEarly Autism Red Flags Infants Toddlers PreschoolersHemant KumarNo ratings yet
- OT For Children With ADHDDocument12 pagesOT For Children With ADHDBeatrizIgelmo100% (1)
- Sensory Diet 2Document2 pagesSensory Diet 2Pamm50% (2)
- sp2 Child Full Assessment Sample PDFDocument15 pagessp2 Child Full Assessment Sample PDFLalit Mittal100% (2)
- Sensory ProfileDocument8 pagesSensory ProfilenymommyNo ratings yet
- PD Sensory Room TrainingDocument35 pagesPD Sensory Room Trainingapi-393264699No ratings yet
- AutismMotorSkillEvaluationFINALBESt028.8 27 09Document6 pagesAutismMotorSkillEvaluationFINALBESt028.8 27 09Shayne Tee-MelegritoNo ratings yet
- R It by Brooke IngersollDocument16 pagesR It by Brooke IngersollJuliana BravoNo ratings yet
- Sensory Profile: Submitted By-Amandeep Kaur M.O.T-Neuro, Sem 3 ENROLLMENT NO - A138141620004 Guided by - Ruby Ma'AmDocument42 pagesSensory Profile: Submitted By-Amandeep Kaur M.O.T-Neuro, Sem 3 ENROLLMENT NO - A138141620004 Guided by - Ruby Ma'Amamandeep kaur100% (1)
- Kathryn Edmands The Impact of Sensory ProcessingDocument26 pagesKathryn Edmands The Impact of Sensory ProcessingBojana VulasNo ratings yet
- TACTILE AND PROPRIOCEPTIVE INTERVENTIONDocument13 pagesTACTILE AND PROPRIOCEPTIVE INTERVENTIONAnup Pednekar100% (1)
- The Effect of A Two-Week Sensory Diet On Fussy Infants With Regulatory SensDocument8 pagesThe Effect of A Two-Week Sensory Diet On Fussy Infants With Regulatory Sensapi-238703581No ratings yet
- Allen Cogntive Disabilties ModelDocument29 pagesAllen Cogntive Disabilties ModelSarah Lyn White-Cantu100% (1)
- Occupational Therapy Sensory Integration Protocol For Early InterDocument56 pagesOccupational Therapy Sensory Integration Protocol For Early Intermanali vyasNo ratings yet
- Fine Motor and Handwriting Skills ActivitiesDocument4 pagesFine Motor and Handwriting Skills Activitiesehopkins5_209No ratings yet
- Caregiver Sensory ProfileDocument6 pagesCaregiver Sensory ProfileRomysah Farooq100% (1)
- Sensory Diet Sample FormatDocument1 pageSensory Diet Sample FormatBernard CarpioNo ratings yet
- Azzam Scale in Practical Guide of Occupational TherapyFrom EverandAzzam Scale in Practical Guide of Occupational TherapyNo ratings yet
- Sensorimotor History Questionnaire For Parents of PreschoolDocument77 pagesSensorimotor History Questionnaire For Parents of Preschoolscribdmuthu100% (2)
- Infant Toddler Sensory Profile Assessment GuideDocument21 pagesInfant Toddler Sensory Profile Assessment GuideFedora Margarita Santander CeronNo ratings yet
- Sensory Integration: A Practical Look at The Theory and Model For Intervention by Megan Carrick, MOTR/LDocument6 pagesSensory Integration: A Practical Look at The Theory and Model For Intervention by Megan Carrick, MOTR/LautismoneNo ratings yet
- CHAPTERIDocument13 pagesCHAPTERIGuess WhoNo ratings yet
- Samsung Marketing Strategy ThesisDocument7 pagesSamsung Marketing Strategy Thesisdeborahquintanaalbuquerque100% (2)
- Teacher EducationDocument112 pagesTeacher EducationhurshawkNo ratings yet
- Sample Research ProtocolDocument5 pagesSample Research Protocollpolvorido100% (1)
- Thesis Sa PagnenegosyoDocument6 pagesThesis Sa PagnenegosyoBuyACollegePaperSingapore100% (2)
- Guidelines For Smart Grid Cyber Security: Vol. 2, Privacy and The Smart GridDocument69 pagesGuidelines For Smart Grid Cyber Security: Vol. 2, Privacy and The Smart GridInterSecuTechNo ratings yet
- The Complete List of Branding Services and Deliverables - CannyDocument15 pagesThe Complete List of Branding Services and Deliverables - CannyBGC MarcomNo ratings yet
- Mallory Brown: (727) 742-9743 - Brown - Mall@husky - Neu.eduDocument1 pageMallory Brown: (727) 742-9743 - Brown - Mall@husky - Neu.eduapi-455273982No ratings yet
- EU-SPRI Conference Proceedings Risk Climate Innovation LinkDocument7 pagesEU-SPRI Conference Proceedings Risk Climate Innovation LinkMD. Naimul Isalm ShovonNo ratings yet
- THR Rolr Halal Science (Aliyah)Document22 pagesTHR Rolr Halal Science (Aliyah)Maisaroh AliyahNo ratings yet
- Trying Lemongrass As Organic Mosquito RepellentDocument41 pagesTrying Lemongrass As Organic Mosquito RepellentSan Shine100% (1)
- ARDI Actors Resources Dynamics I PDFDocument14 pagesARDI Actors Resources Dynamics I PDFMarcela BasurtoNo ratings yet
- A Study On Budgetory ControlDocument39 pagesA Study On Budgetory ControlStella PaulNo ratings yet
- I and S - Guide New-2014-15Document69 pagesI and S - Guide New-2014-15Llama jennerNo ratings yet
- Eco TectureDocument20 pagesEco TectureMichael Jherome NuqueNo ratings yet
- Moreno MethodologyDocument97 pagesMoreno MethodologyUyên TrươngNo ratings yet
- Group 1 Rose Research JournalDocument8 pagesGroup 1 Rose Research JournalJoyce NoblezaNo ratings yet
- Photo-Elicitation Interview - 2004-Clark-IbáÑez-1507-27Document21 pagesPhoto-Elicitation Interview - 2004-Clark-IbáÑez-1507-27Fidel Terenciano FilhoNo ratings yet
- Rendang Malaysia - Culinary Heritage and Cultural IdentityDocument2 pagesRendang Malaysia - Culinary Heritage and Cultural Identitynajwalai98No ratings yet
- Template of JournalDocument6 pagesTemplate of JournalArisYamanNo ratings yet
- Vels University MBA Logistics & Shipping Management Program OutcomesDocument116 pagesVels University MBA Logistics & Shipping Management Program OutcomesDhanashekar NaiduNo ratings yet
- Boncodin MatrixDocument3 pagesBoncodin Matrixlindsay boncodinNo ratings yet
- Book Catalogue 2021Document79 pagesBook Catalogue 2021navecNo ratings yet
- Challenging ocular architecture with multi-sensory designDocument4 pagesChallenging ocular architecture with multi-sensory designayush datta100% (1)
- Babixxx 170713 1Document12 pagesBabixxx 170713 1Nelson PutraNo ratings yet
- Population and SampleDocument10 pagesPopulation and SampleTata Intan TamaraNo ratings yet
- RESEARCH PROPOSAL FORMAT - June 20 2023Document5 pagesRESEARCH PROPOSAL FORMAT - June 20 2023Saikawa YuukiNo ratings yet
- Inventory Control Methods for Apparel IndustryDocument3 pagesInventory Control Methods for Apparel IndustryARPITA PATHYNo ratings yet
- Literature Review Strategic Planning and PerformanceDocument4 pagesLiterature Review Strategic Planning and Performancec5qvf1q1No ratings yet
- BRUNBORG Et Al-2011-Journal of Sleep ResearchDocument7 pagesBRUNBORG Et Al-2011-Journal of Sleep ResearchAndhika CahyaNo ratings yet