You might also like
- C C CC C ! ! ! !!! ! !"#$"% C C & C' (!) CDocument13 pagesC C CC C ! ! ! !!! ! !"#$"% C C & C' (!) Charshna_20No ratings yet
- Work Life BalanceDocument7 pagesWork Life BalanceAshwin KunderNo ratings yet
- Questionnaire: Work Life BalanceDocument3 pagesQuestionnaire: Work Life BalanceAnupam DasNo ratings yet
- Questionnaire On Work - Life BalanceDocument4 pagesQuestionnaire On Work - Life BalanceSakshi SharmaNo ratings yet
- Questionnaire On Work Life BalanceDocument6 pagesQuestionnaire On Work Life BalanceMahesh SharmaNo ratings yet
- Final Correction QuestionnaireDocument3 pagesFinal Correction QuestionnairePrudvi ReddyNo ratings yet
- A Study On Motivation Among The Employees QuestionerDocument6 pagesA Study On Motivation Among The Employees QuestionerkarthikeyanNo ratings yet
- Workplace Wellbeing QueDocument5 pagesWorkplace Wellbeing QueRavi KoniNo ratings yet
- How to Manage Problem Employees: A Step-by-Step Guide for Turning Difficult Employees into High PerformersFrom EverandHow to Manage Problem Employees: A Step-by-Step Guide for Turning Difficult Employees into High PerformersRating: 4 out of 5 stars4/5 (1)
- Questionnaire On Work Life BalanceDocument5 pagesQuestionnaire On Work Life BalanceSabin Shrestha100% (1)
- Work Life Balance QuestionnaireDocument4 pagesWork Life Balance QuestionnaireBanana Q100% (3)
- Fathers and Paid Work - Sample Questionnaire: What Is Work Life Balance?Document8 pagesFathers and Paid Work - Sample Questionnaire: What Is Work Life Balance?naveenhinniNo ratings yet
- Work Life Balance QuestionnaireDocument4 pagesWork Life Balance QuestionnaireIndu SumeshNo ratings yet
- Work-Life Balance With Focus On Family LifeDocument31 pagesWork-Life Balance With Focus On Family LifeJames Farrugia100% (1)
- Achieving Work-Life Balance by Knowing The Right PrioritiesDocument2 pagesAchieving Work-Life Balance by Knowing The Right PrioritiesLuis Lorenzo AfricaNo ratings yet
- Questionnaire On Work Life Balance For Working ParentsDocument3 pagesQuestionnaire On Work Life Balance For Working ParentsJithin BenedictNo ratings yet
- Work Life BalanceDocument24 pagesWork Life Balancedevyani saxena100% (2)
- Questionnaire On Work Life Balance For Working ParentsDocument3 pagesQuestionnaire On Work Life Balance For Working ParentsEureka KashyapNo ratings yet
- Work-Life Balance Full ReportDocument178 pagesWork-Life Balance Full ReportBen HarveyNo ratings yet
- The Impact of Working Life and Personal Life Balance in An Organizational Environment: A Review PaperDocument6 pagesThe Impact of Working Life and Personal Life Balance in An Organizational Environment: A Review PaperInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Achieving Work-Life BalanceDocument30 pagesAchieving Work-Life Balancemando HussienNo ratings yet
- Questionnaire On Job SatisfactionDocument8 pagesQuestionnaire On Job SatisfactionningegowdaNo ratings yet
- Study On Work-Life Balance - Need and Imperatives As An HR Initiative in Candid Bpo ServicesDocument56 pagesStudy On Work-Life Balance - Need and Imperatives As An HR Initiative in Candid Bpo ServicesDeepak SinghalNo ratings yet
- Work Life Balance Questionnaire PDFDocument4 pagesWork Life Balance Questionnaire PDFAyu RadityaNo ratings yet
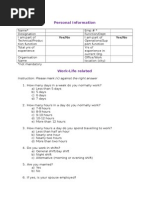
- Personal Information: Name (Optional) : Gender: Age Group: 26 Qualification: UG PG Experience: 6 SalaryDocument3 pagesPersonal Information: Name (Optional) : Gender: Age Group: 26 Qualification: UG PG Experience: 6 Salaryspsurya2013No ratings yet
- Questionnaire Business ResearchDocument9 pagesQuestionnaire Business ResearchjebatmalanglagiNo ratings yet
- Job Satisfaction Questionnaire PDFDocument3 pagesJob Satisfaction Questionnaire PDFShibu ThakurNo ratings yet
- Corporate Social Responsibility: Case Studies OnDocument31 pagesCorporate Social Responsibility: Case Studies OnJIRRARAJIV100% (1)
- Work Life IntegrationDocument10 pagesWork Life IntegrationKrutika AshtikarNo ratings yet
- Work-Life Integration Experiences of Mid-Career PRDocument25 pagesWork-Life Integration Experiences of Mid-Career PRWawan PrasetyoNo ratings yet
- Part2 Work-Life BalanceDocument74 pagesPart2 Work-Life BalanceBhuvanesh Raam100% (2)
- Kabsy Consultancy Servicesstaff PoliciesDocument22 pagesKabsy Consultancy Servicesstaff PoliciesEvangelist Kabaso SydneyNo ratings yet
- Total Compensation Strategy Presentation SlideDocument26 pagesTotal Compensation Strategy Presentation SlideJahid HasanNo ratings yet
- Job SatisfactionDocument2 pagesJob Satisfactionsantosh_sahoo659473No ratings yet
- Sumit Final Project of Work Life BalanceDocument102 pagesSumit Final Project of Work Life BalancetejasNo ratings yet
- Performance ManagentDocument43 pagesPerformance ManagentMoshiur Tusher0% (1)
- Managing Talent & Careers & Succession Planning - Group 10Document63 pagesManaging Talent & Careers & Succession Planning - Group 10Neha SabnisNo ratings yet
- Questionnaire Fringe BenefitsDocument4 pagesQuestionnaire Fringe BenefitsNeha AroraNo ratings yet
- Questionnaire Layout Total Questions in A Questionnaire: Minimum 15Document18 pagesQuestionnaire Layout Total Questions in A Questionnaire: Minimum 15suman v bhatNo ratings yet
- Report On Stress in OrganizationDocument12 pagesReport On Stress in OrganizationRanjeet Kumar SinghNo ratings yet
- Work Life Balance QuestionnaireDocument4 pagesWork Life Balance QuestionnaireSurbhi Sharma0% (1)
- Work Life BalanceDocument41 pagesWork Life Balancekarnarc0% (1)
- Job SatisfactionDocument2 pagesJob SatisfactionJutt SmithNo ratings yet
- CH 9 Orientation Placement SeprationDocument26 pagesCH 9 Orientation Placement SeprationabidNo ratings yet
- Work Life Balance QuestionnareDocument2 pagesWork Life Balance QuestionnareDr-Shefali Garg100% (1)
- Article On Recruitment & Selection Process in NGODocument7 pagesArticle On Recruitment & Selection Process in NGOrahat ahmedNo ratings yet
- Organizational Atmosphere SurveyDocument4 pagesOrganizational Atmosphere Surveycesar_augusto_agsNo ratings yet
- Arun ProjectDocument61 pagesArun ProjectPrathish JosephNo ratings yet
- Sample Criteria For Job EvaluationDocument9 pagesSample Criteria For Job EvaluationGabriel AdoraNo ratings yet
- Characteristics of Employee BenefitsDocument4 pagesCharacteristics of Employee BenefitsMaitreyee Paralkar-VichareNo ratings yet
- Work Life BalanceDocument16 pagesWork Life BalanceChandrashekharCSKNo ratings yet
- Work Life Balance QuestionnaireDocument7 pagesWork Life Balance Questionnairechirag bhojakNo ratings yet
- Talent Management Strategy 3 1Document18 pagesTalent Management Strategy 3 1Farhan Rahman ArnobNo ratings yet
- Dear Respondent, This Questionnaire Is Designed To Collect Data of Population of Employees ForDocument2 pagesDear Respondent, This Questionnaire Is Designed To Collect Data of Population of Employees ForAmina RizwanNo ratings yet
- Induction/Orientation & PlacementDocument17 pagesInduction/Orientation & Placementvivek kumarNo ratings yet
- Succession Planning: "Thinking About Tomorrow Today"Document4 pagesSuccession Planning: "Thinking About Tomorrow Today"yogesh verma100% (1)
- Job Satisfaction Survey TemplateDocument2 pagesJob Satisfaction Survey TemplateCherry Mae L. VillanuevaNo ratings yet
- Presentation On LeadershipDocument25 pagesPresentation On Leadershipruchi goelNo ratings yet
- A Project Report ON Work Life BalanceDocument21 pagesA Project Report ON Work Life BalanceSaumya Ranjan ChoudhuryNo ratings yet
- John Maxwell On LeadershipDocument9 pagesJohn Maxwell On LeadershipRobert DechosNo ratings yet
- Fullsize SBAR Report SheetDocument1 pageFullsize SBAR Report SheetShane LambertNo ratings yet
- Fucidin® OintDocument1 pageFucidin® OintIanthe SinghNo ratings yet
- SofradexDocument3 pagesSofradexWahidNo ratings yet
- Jurnal OnlineDocument5 pagesJurnal OnlineWireifnitedNo ratings yet
- Game-Based Cognitive-Behavioral Therapy (GB-CBT) LEER PDFDocument7 pagesGame-Based Cognitive-Behavioral Therapy (GB-CBT) LEER PDFkarenNo ratings yet
- Tennis Elbow' or Lateral Epicondylitis: Information For YouDocument4 pagesTennis Elbow' or Lateral Epicondylitis: Information For YouvivinNo ratings yet
- Opinion WritingDocument20 pagesOpinion WritingnirmalaNo ratings yet
- 220200320sathiya PrakashDocument95 pages220200320sathiya Prakashpriya selvaraj100% (1)
- Mudra PDFDocument9 pagesMudra PDFKr SelvakumarNo ratings yet
- Bacteriological Quality of Street Vended Food PanipuriDocument5 pagesBacteriological Quality of Street Vended Food PanipuriYus EfendiNo ratings yet
- QUESTIONNAIREDocument3 pagesQUESTIONNAIREKatherine Aplacador100% (4)
- DotDocument2 pagesDotahsanraja123No ratings yet
- History of SensorDocument37 pagesHistory of SensornsdewNo ratings yet
- Pregnancy Induced HypertensionDocument16 pagesPregnancy Induced Hypertensiondgraham36No ratings yet
- Prepared by Muhammad Salman: This Brand Plan Has Been Designed For The ProductDocument90 pagesPrepared by Muhammad Salman: This Brand Plan Has Been Designed For The ProductMuhammad SalmanNo ratings yet
- T 1234029783 11845985 Nursing Crib Com Nursing Care Plan Dengue FeverDocument2 pagesT 1234029783 11845985 Nursing Crib Com Nursing Care Plan Dengue Feversamantha cortezNo ratings yet
- Get in Shape Month2Document5 pagesGet in Shape Month2Caroline Sandry100% (1)
- Ayurveda Treatment SkinDocument4 pagesAyurveda Treatment SkinAkash SharmaNo ratings yet
- Aubf Chemical Examination Credits To The OwnerDocument19 pagesAubf Chemical Examination Credits To The Ownerchippai100% (2)
- URINARY SYSTEM 1 Copyright RevisedDocument5 pagesURINARY SYSTEM 1 Copyright RevisedSherida GibbsNo ratings yet
- Orotol Plus GB 0118Document16 pagesOrotol Plus GB 0118rahmatNo ratings yet
- At The Doctor's: Speaker 1: I've Just Had AnDocument2 pagesAt The Doctor's: Speaker 1: I've Just Had AnVictor0% (1)
- Autonomic Nervous System: Rodina Rivera-Gorospe, M.DDocument44 pagesAutonomic Nervous System: Rodina Rivera-Gorospe, M.DPogo LocoNo ratings yet
- Home Private ServiceDocument4 pagesHome Private ServiceTubagus Adil AL AminNo ratings yet
- Observator Ios 2016Document355 pagesObservator Ios 2016ajgamesNo ratings yet
- ARTICLE - DR.S R PHATAK. Kinjal Dave - 4th BHMCDocument2 pagesARTICLE - DR.S R PHATAK. Kinjal Dave - 4th BHMCᎧᎷ ᎴᏗᏉᏋNo ratings yet
- 16-4 I The Truth About Physician Health ProgramsDocument5 pages16-4 I The Truth About Physician Health ProgramslbandrewNo ratings yet
- Cancer PainDocument52 pagesCancer PainIndraYudhi100% (1)
- Congenital HypothyroidismDocument36 pagesCongenital HypothyroidismRandi DwiyantoNo ratings yet
- L10 ToleranceDocument19 pagesL10 Tolerancesara garciaNo ratings yet