You might also like
- Perfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationFrom EverandPerfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationRating: 5 out of 5 stars5/5 (2)
- DMDudzinski EKG Algorithm4Document1 pageDMDudzinski EKG Algorithm4nate simmons100% (1)
- Lecture Notes On CardiologyDocument31 pagesLecture Notes On CardiologyambiskuysNo ratings yet
- RHC in PH FinalDocument36 pagesRHC in PH FinalKirti KadianNo ratings yet
- CCC Nurs 235 - Pediatric & Maternity NursingFinal Study GuideDocument13 pagesCCC Nurs 235 - Pediatric & Maternity NursingFinal Study GuideHeidi HeffelfingerNo ratings yet
- Cardiovascular Sequence, October 2000: A Wave in Atrial PressureDocument5 pagesCardiovascular Sequence, October 2000: A Wave in Atrial PressureMohamed KhattabNo ratings yet
- FA 2020 - Cardio Sterling Curve PDFDocument15 pagesFA 2020 - Cardio Sterling Curve PDFDrbee10No ratings yet
- CCRN CardiacDocument39 pagesCCRN CardiacMike100% (5)
- Clinical Congenital Heart Disease: Prof M S Ranjit MD DCH Senior Consultant Paed. Cardiologist ChennaiDocument78 pagesClinical Congenital Heart Disease: Prof M S Ranjit MD DCH Senior Consultant Paed. Cardiologist ChennaiAnişoara FrunzeNo ratings yet
- Congenital Heart Diseases ReviewDocument2 pagesCongenital Heart Diseases ReviewQworldNo ratings yet
- Downloadfile 28Document31 pagesDownloadfile 28Chowdhury Mohammed Tawhid TasneefNo ratings yet
- Ebook Hupperts Notes Pathophysiology and Clinical Pearls For Internal Medicine PDF Full Chapter PDFDocument67 pagesEbook Hupperts Notes Pathophysiology and Clinical Pearls For Internal Medicine PDF Full Chapter PDFmartha.delancey633100% (26)
- CCRN-PCCN-CMC Review Cardiac Part 3Document18 pagesCCRN-PCCN-CMC Review Cardiac Part 3Giovanni MictilNo ratings yet
- FP-C ReviewDocument71 pagesFP-C ReviewJamesNo ratings yet
- ABA OSCE ReviewDocument25 pagesABA OSCE ReviewJohn Smith100% (1)
- Hupperts Notes Pathophysiology and Clinical Pearls For Internal Medicine Laura Huppert Full ChapterDocument67 pagesHupperts Notes Pathophysiology and Clinical Pearls For Internal Medicine Laura Huppert Full Chapterannette.reese953100% (6)
- Httpsboardsandbeyoend Image.s3.Us East 1.amazonaws - compublicdocumentsStep1SlidesCardiologySlides2021 FullSize 3 PDFDocument1,036 pagesHttpsboardsandbeyoend Image.s3.Us East 1.amazonaws - compublicdocumentsStep1SlidesCardiologySlides2021 FullSize 3 PDFcnikhila93No ratings yet
- CARDIODocument10 pagesCARDIOMarcel TabucolNo ratings yet
- High Yield Surgery Shelf Exam Review CompleteDocument10 pagesHigh Yield Surgery Shelf Exam Review CompleteAmir Ali100% (1)
- Hemodynamic Failure March 2016Document61 pagesHemodynamic Failure March 2016Adriana VillarrealNo ratings yet
- Review of HD Monitoring: DR Ghaleb Almekhlafi MD, SFCCM, EdicDocument105 pagesReview of HD Monitoring: DR Ghaleb Almekhlafi MD, SFCCM, EdicGHALEB A. Almekhlafi100% (1)
- Notes To RewriteDocument6 pagesNotes To RewriteEunice Angela FulguerasNo ratings yet
- Clin Med For PAsDocument32 pagesClin Med For PAsMaryNguyen100% (2)
- Swan Ganz FinalDocument36 pagesSwan Ganz FinalDanial HassanNo ratings yet
- Septic Shock: Mixed Venous Oxygen Saturation IncreasedDocument1 pageSeptic Shock: Mixed Venous Oxygen Saturation IncreasedAsfand Yar KakarNo ratings yet
- Ankle Brachial Index, RandomDocument4 pagesAnkle Brachial Index, Randomkabal321No ratings yet
- Physiology Slides UsmleDocument46 pagesPhysiology Slides Usmlejustseas100% (1)
- Hemodynamic MonitoringDocument33 pagesHemodynamic MonitoringISICLE GTNo ratings yet
- Shock States Topic DiscussionDocument3 pagesShock States Topic Discussionapi-648891519No ratings yet
- Hemodinamik Dasar Invasive 2Document27 pagesHemodinamik Dasar Invasive 2Tkv UhamkaNo ratings yet
- LVEDP TableDocument3 pagesLVEDP TablehollyuNo ratings yet
- Cardiovascular System ConditionsDocument4 pagesCardiovascular System ConditionsNinjaNo ratings yet
- Cardiology-3 HFDocument17 pagesCardiology-3 HFMahmoud RamadanNo ratings yet
- 6 CVS RegulationDocument55 pages6 CVS RegulationDisha SuvarnaNo ratings yet
- Medsurg NursingDocument3 pagesMedsurg NursingGeraldine TeneclanNo ratings yet
- System and Disease III ComprehensiveDocument46 pagesSystem and Disease III Comprehensivenasr234No ratings yet
- Pulmonary Artery Catheters and Hemodynamic MonitoringDocument32 pagesPulmonary Artery Catheters and Hemodynamic Monitoringjpsahni100% (1)
- Stenotic Lesions AaDocument7 pagesStenotic Lesions Aaprem kotiNo ratings yet
- Copy Monitoring HemodinamicDocument23 pagesCopy Monitoring HemodinamicwarmanlicyNo ratings yet
- EKG Interpretation NursingDocument14 pagesEKG Interpretation NursingTanya ViarsNo ratings yet
- PcicardDocument2 pagesPcicardWahdat100% (1)
- Hemodynamic MonitoringDocument41 pagesHemodynamic MonitoringSuresh KumarNo ratings yet
- MS4 Exam 2Document27 pagesMS4 Exam 2JessNo ratings yet
- ECG at A GlanceDocument53 pagesECG at A GlancePetrus TjiangNo ratings yet
- Ntiarrhythmic X: Use Mechanism of Action Toxicities NotesDocument3 pagesNtiarrhythmic X: Use Mechanism of Action Toxicities NotesthescarletpimpernelsNo ratings yet
- Cardiology CardiovascularExaminationDocument5 pagesCardiology CardiovascularExaminationSalifyanji SimpambaNo ratings yet
- Path of Blood FlowDocument10 pagesPath of Blood Flowkiki188No ratings yet
- Code Mnagment Repaired FEB 1 2017Document22 pagesCode Mnagment Repaired FEB 1 2017Mr. Tauqeer Ahmed Faculty Member FUCNNo ratings yet
- ECG Interpretation and Dysrhythmias: Karen L. O'Brien MSN, RN JAN 07Document60 pagesECG Interpretation and Dysrhythmias: Karen L. O'Brien MSN, RN JAN 07ampogison08No ratings yet
- 04-Role of Echo in Pulm Hypertion N EmbolismDocument57 pages04-Role of Echo in Pulm Hypertion N EmbolismSiska Istanah Wong SintingNo ratings yet
- Cardiac Study GuideDocument3 pagesCardiac Study GuideLindsay BirnbrichNo ratings yet
- NCLEX Cram SheetDocument6 pagesNCLEX Cram Sheetaishwariyapokharel55No ratings yet
- Blood Pressure Regulation MechanismsDocument68 pagesBlood Pressure Regulation MechanismsPhysiology by Dr RaghuveerNo ratings yet
- Hemodynamic MonitoringDocument111 pagesHemodynamic MonitoringVenkatesan AnnamalaiNo ratings yet
- Rosenberg Circulatory Assist DevicesDocument61 pagesRosenberg Circulatory Assist DevicesMilisha Albro100% (1)
- Cardio Pulmonary Final FrontierDocument10 pagesCardio Pulmonary Final Frontierdina sharafNo ratings yet
- Anatomy: Cardiac Symptoms Cardiac Examination ECG and X RayDocument27 pagesAnatomy: Cardiac Symptoms Cardiac Examination ECG and X RayEmey AlahmadNo ratings yet
- Cardiovascular SystemDocument24 pagesCardiovascular SystemCandice100% (1)
- Swan Gantz Catherter and The Meaning of Its ReadingsDocument67 pagesSwan Gantz Catherter and The Meaning of Its ReadingsNouman Hameed100% (1)
- BOC Clinical Chemistry ReviewDocument6 pagesBOC Clinical Chemistry ReviewBloody MarieNo ratings yet
- Introduction To ElectrolytesDocument13 pagesIntroduction To ElectrolytesMaam ShaNo ratings yet
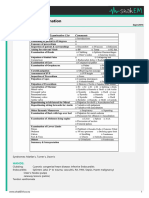
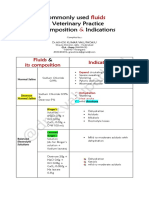
- Common IV Fluids at Composition & IndicationsDocument2 pagesCommon IV Fluids at Composition & IndicationsNilesh SuryawanshiNo ratings yet
- NCM 109 Finals NotesDocument21 pagesNCM 109 Finals NotesERIKA BOOTS CABALUNANo ratings yet
- Medical Surgical Nursing Cardio Vascular System ClassDocument15 pagesMedical Surgical Nursing Cardio Vascular System Classvallal100% (2)
- Lactic Acidosis and The Role of Sodium Bicarbonate: A Narrative Opinion Running Head: Lactic Acidosis and Sodium BicarbonateDocument38 pagesLactic Acidosis and The Role of Sodium Bicarbonate: A Narrative Opinion Running Head: Lactic Acidosis and Sodium BicarbonatentnquynhproNo ratings yet
- Chemistry: 25 Minutes 30 QuestionsDocument22 pagesChemistry: 25 Minutes 30 QuestionsAlex OlivarNo ratings yet
- NCLEX Study Notes 20080924Document61 pagesNCLEX Study Notes 20080924Shan Shan He100% (6)
- Abg Quiz in Class With Answers 1Document3 pagesAbg Quiz in Class With Answers 1Janae TaylorNo ratings yet
- Comp ReDocument9 pagesComp ReleninisanurseNo ratings yet
- NCM 112Document24 pagesNCM 112Amoroso, Marian Corneth D.No ratings yet
- 5 6231171839033344436Document454 pages5 6231171839033344436Amit KumarNo ratings yet
- Associations USMLEDocument99 pagesAssociations USMLEnu.bombinaNo ratings yet
- Acid Base ImbalancesDocument7 pagesAcid Base ImbalancesNicholas TagleNo ratings yet
- Fluid, Electrolyte, and Acid-BaseDocument6 pagesFluid, Electrolyte, and Acid-BaseRaquel MonsalveNo ratings yet
- Salicylates Tca ToxicityDocument54 pagesSalicylates Tca Toxicityapi-298936498No ratings yet
- All FormulasDocument3 pagesAll FormulasKevin Apeles100% (1)
- Acid-Base Balance: Graciela Lou F. Mana-Ay, RN, ManDocument68 pagesAcid-Base Balance: Graciela Lou F. Mana-Ay, RN, ManKeshia Joyce LimNo ratings yet
- Metabolic Encephalopaty PDFDocument46 pagesMetabolic Encephalopaty PDFRez QNo ratings yet
- DocxDocument99 pagesDocxVanessa AbboudNo ratings yet
- Medical Surgical Nursing ReviewDocument16 pagesMedical Surgical Nursing ReviewArda LynNo ratings yet
- Mcqs Fcps Feb 2018 Evening ShiftDocument20 pagesMcqs Fcps Feb 2018 Evening ShiftDrAttaullah ArbaniNo ratings yet
- Fundamentals of NursingDocument13 pagesFundamentals of NursingGiselle Chloe Baluya icoNo ratings yet
- Aspirin OverdoseDocument3 pagesAspirin OverdoseSaputra BismaNo ratings yet
- Interpretation of The Abnormal Laboratory Test .2Document11 pagesInterpretation of The Abnormal Laboratory Test .2Justine DumaguinNo ratings yet
- MK Combined PDFDocument93 pagesMK Combined PDFAnkit ChoudharyNo ratings yet
- Old Free 120 - Answers & Explanations (SP)Document63 pagesOld Free 120 - Answers & Explanations (SP)abdulahad mohamedNo ratings yet
- ShockDocument177 pagesShockISMAIL100% (1)
- Me Pediatrics Ntruhs Previous Question Papers Chapter WiseDocument9 pagesMe Pediatrics Ntruhs Previous Question Papers Chapter WiseNarendra AnnaladasuNo ratings yet
- Concept Map FinalDocument5 pagesConcept Map Finalapi-545001894No ratings yet