You might also like
- BandagingDocument12 pagesBandagingJUANJOSEFOXNo ratings yet
- Definition of BandagingDocument18 pagesDefinition of Bandagingvkshamini91604250% (2)
- BandagesDocument39 pagesBandages4LetterLie31100% (1)
- Bandaging (Handouts)Document55 pagesBandaging (Handouts)Cik AmoiNo ratings yet
- BandagingDocument6 pagesBandagingwinkerbellNo ratings yet
- BandagingDocument46 pagesBandagingDr. Jayesh Patidar100% (1)
- BandagingDocument25 pagesBandagingsusie eusebius mudi100% (1)
- Bandaging GNMDocument46 pagesBandaging GNMjoslinjohn100% (2)
- Application of Bandages and Binders - StudentsDocument110 pagesApplication of Bandages and Binders - Studentsjeremiah90% (10)
- Bandaging & SplintingDocument22 pagesBandaging & SplintingGemmith Gosanes100% (1)
- Body Mechanics and Transferring PatientDocument57 pagesBody Mechanics and Transferring PatientRhenier S. Ilado100% (2)
- 5.casts and MoldsDocument30 pages5.casts and MoldsKatrina PonceNo ratings yet
- BANDAGING ProcedureDocument6 pagesBANDAGING ProcedureAngelie PantajoNo ratings yet
- Prepared By: Anne Jillian T. Singson, RN, MN: (Assisting Clients in The Use of Assistive Ambulatory Devices)Document22 pagesPrepared By: Anne Jillian T. Singson, RN, MN: (Assisting Clients in The Use of Assistive Ambulatory Devices)Jan Federick Bantay100% (1)
- WALKING AIDS (Assistive Devices) : College of NursingDocument15 pagesWALKING AIDS (Assistive Devices) : College of NursingJojo JustoNo ratings yet
- Bandaging TechniqueDocument5 pagesBandaging TechniqueLoren GayudanNo ratings yet
- Procedure in Preparing Patient To Move From BedDocument1 pageProcedure in Preparing Patient To Move From BedcrrfrncNo ratings yet
- Checklists For Transfer and AmbulationDocument15 pagesChecklists For Transfer and Ambulationmido100% (1)
- Bandaging TechniquesDocument4 pagesBandaging TechniqueshgfhfghfghgNo ratings yet
- BandagingDocument2 pagesBandagingA CNo ratings yet
- BANDAGING Powerpoint 1Document30 pagesBANDAGING Powerpoint 1Maria Eloisa Junelle O. Nacawili0% (1)
- BandagingDocument78 pagesBandagingRichelle Almonte100% (2)
- Different Operating Room InstrumentDocument4 pagesDifferent Operating Room InstrumentMaikka Kyril Abarquez50% (2)
- Positioning and Draping ChecklistDocument5 pagesPositioning and Draping ChecklistSean HolarNo ratings yet
- Script For Female CatheterizationDocument3 pagesScript For Female CatheterizationMacy Marquez100% (1)
- Transfer Techniques & Immobilization TechniquesDocument29 pagesTransfer Techniques & Immobilization TechniquesRegina Garrard100% (3)
- Fracture (Cast Care)Document6 pagesFracture (Cast Care)Vane UcatNo ratings yet
- Surgical Instruments: Grasping and Clamping Retracting Cutting and Dissecting Probing and DilatingDocument55 pagesSurgical Instruments: Grasping and Clamping Retracting Cutting and Dissecting Probing and DilatingCathreen Agatha Fule100% (2)
- Surgical Gowning and GlovingDocument15 pagesSurgical Gowning and GlovingAllyssa MackinnonNo ratings yet
- Splints and Casts Indications and MethodsDocument9 pagesSplints and Casts Indications and MethodsJay GaneshNo ratings yet
- Transfer TechniquesDocument5 pagesTransfer TechniquesJan Jamison Zulueta100% (1)
- Skin PreparationDocument3 pagesSkin Preparationmckulit_joey100% (2)
- Procedure in Turning Client To Side-Lying PositionDocument1 pageProcedure in Turning Client To Side-Lying PositioncrrfrncNo ratings yet
- NCM Checklist - Occupied and Unoccupied BedDocument6 pagesNCM Checklist - Occupied and Unoccupied BedYanna Habib-MangotaraNo ratings yet
- Feeding Via Gastric GavageDocument3 pagesFeeding Via Gastric Gavageneleh gray0% (1)
- Geriatric Assistive DevicesDocument26 pagesGeriatric Assistive DevicesBrixter Greyson SencronoNo ratings yet
- Transfer of A PatientDocument8 pagesTransfer of A Patienttrupti patelNo ratings yet
- Mobility and ImmobilityDocument37 pagesMobility and ImmobilityAndrea Huecas Tria100% (2)
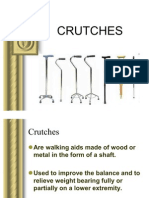
- CRUTCHESDocument35 pagesCRUTCHESBebing CostinianoNo ratings yet
- Fundamental of NursingDocument1 pageFundamental of Nursingioana_ciobincanNo ratings yet
- Skin TractionDocument10 pagesSkin Tractionpritinez2516100% (1)
- NCM Lab Checklist - PositioningDocument2 pagesNCM Lab Checklist - PositioningYanna Habib-MangotaraNo ratings yet
- Unit 1: Concepts, Principles, and Theories in The Care of Older AdultsDocument10 pagesUnit 1: Concepts, Principles, and Theories in The Care of Older AdultsEricson CandelariaNo ratings yet
- Surgical InstrumentsDocument6 pagesSurgical Instrumentsgeorgeloto12No ratings yet
- Management of Clients With Burns and ShockDocument7 pagesManagement of Clients With Burns and ShockJunah Marie Rubinos Palarca0% (1)
- Traction NursingDocument75 pagesTraction NursingSujith KuttanNo ratings yet
- Bandaging and SplintingDocument2 pagesBandaging and Splintinglovemaeus6797No ratings yet
- Lifts and CarriesDocument7 pagesLifts and CarriesDel Mabel100% (1)
- Lab Clin Clin Tasks Attempted 1 2 3 4 5 6 7: ST ND RD TH TH TH THDocument4 pagesLab Clin Clin Tasks Attempted 1 2 3 4 5 6 7: ST ND RD TH TH TH THRichard Patterson100% (1)
- Assist With Client or Patient MovementDocument88 pagesAssist With Client or Patient Movementmihret gashayeNo ratings yet
- BANDAGINGDocument6 pagesBANDAGINGSweet BenitezNo ratings yet
- Myra LevineDocument13 pagesMyra LevineLarra Suzainne Vanguardia FanegaNo ratings yet
- Active and Passive Range of Motion Exercises.Document16 pagesActive and Passive Range of Motion Exercises.Attila Tamas100% (1)
- Assistive Devices For Walking, Casts, and Traction CareDocument7 pagesAssistive Devices For Walking, Casts, and Traction Careアンナドミニク100% (1)
- Traction MethodsDocument11 pagesTraction MethodsalcaponeNo ratings yet
- Patient Positioning: Complete Guide For MidwivesDocument12 pagesPatient Positioning: Complete Guide For MidwivesRohlen BaguioNo ratings yet
- Duties and Responsibilities in or (SCRUB NURSE AND CIRCULATING NURSE) by JheaaDocument5 pagesDuties and Responsibilities in or (SCRUB NURSE AND CIRCULATING NURSE) by JheaaSareno PJhēaNo ratings yet
- BandagesDocument23 pagesBandagesNamikaze Razors SullivanNo ratings yet
- Applying An Elastic Bandage-CheklistDocument4 pagesApplying An Elastic Bandage-CheklistAh AlshaibaniNo ratings yet
- Bandage WrappingDocument8 pagesBandage WrappingzkinnehNo ratings yet
- Instructional Module: Republic of The Philippines Nueva Vizcaya State University Bayombong, Nueva VizcayaDocument7 pagesInstructional Module: Republic of The Philippines Nueva Vizcaya State University Bayombong, Nueva VizcayaAkemi YeonNo ratings yet
- L G 0014511967 0046781894Document26 pagesL G 0014511967 0046781894anggiNo ratings yet
- Reproductive SystemDocument7 pagesReproductive Systemcollege code - 5No ratings yet
- Avian Sensory Systems: Sensory World Similar To Ours, That of Other Primates, Primarily VisualDocument30 pagesAvian Sensory Systems: Sensory World Similar To Ours, That of Other Primates, Primarily VisualijudoptoNo ratings yet
- 2. Atlas of Anatomy. Netter 3. An Atlas Of Surgical Anatomy Masquelet.pdf 4. Anatomie Sрringer.pdf 5. Anatomy Coloring Book Benjamin Cummings PDFDocument2 pages2. Atlas of Anatomy. Netter 3. An Atlas Of Surgical Anatomy Masquelet.pdf 4. Anatomie Sрringer.pdf 5. Anatomy Coloring Book Benjamin Cummings PDFmrmarcoguimaNo ratings yet
- DapusDocument4 pagesDapusRiza ZaharaNo ratings yet
- Rehabilitation After Rotator Cuff RepairDocument22 pagesRehabilitation After Rotator Cuff Repairgaia_ravasio9277100% (2)
- Neuropathy Symptom Score Dan Neuropathy Deficit Score Sebagai Skor Diagnostik Neuropati DiabetikDocument8 pagesNeuropathy Symptom Score Dan Neuropathy Deficit Score Sebagai Skor Diagnostik Neuropati DiabetikmaurinmarceoiaNo ratings yet
- Chapter 12 - HeartDocument3 pagesChapter 12 - HeartAngelyka CabaloNo ratings yet
- Goldenhar SyndromeDocument16 pagesGoldenhar Syndromesaeid seyedraoufiNo ratings yet
- NUR-116 Exam SampleDocument4 pagesNUR-116 Exam SampleOMAR SUDNo ratings yet
- Facial Cupping Gua Sha InstructionsDocument12 pagesFacial Cupping Gua Sha InstructionsJonathan LópezNo ratings yet
- BDS-Batch 11-Module 1 - CA - Anatomy Question BankDocument2 pagesBDS-Batch 11-Module 1 - CA - Anatomy Question BankcheckmateNo ratings yet
- Atlas of Common Subluxations of The Human Spine and Pelvis PDFDocument238 pagesAtlas of Common Subluxations of The Human Spine and Pelvis PDFBruno RavazziNo ratings yet
- Eng-Fil Parts of The BodyDocument14 pagesEng-Fil Parts of The BodyJoseth OyardoNo ratings yet
- Soalan Bio Bab 3 3.1 Ccov20 1Document6 pagesSoalan Bio Bab 3 3.1 Ccov20 1Anas AjmalNo ratings yet
- A Three-Dimensional Biomechanical AnalysisDocument15 pagesA Three-Dimensional Biomechanical AnalysisPaolo SantorumNo ratings yet
- Pulmonary CirculationDocument36 pagesPulmonary CirculationSllavko K. KallfaNo ratings yet
- Cleansing The Limph GlandsDocument2 pagesCleansing The Limph Glandsonkarsingh2100% (2)
- Back Pain PamphletDocument2 pagesBack Pain Pamphletsjeyarajah21No ratings yet
- Dumbbell Step-Up: ExecutionDocument11 pagesDumbbell Step-Up: ExecutionDavid RomeroNo ratings yet
- Materi Dan Latihan Soal Part of BodyDocument2 pagesMateri Dan Latihan Soal Part of BodySeferagic FatihNo ratings yet
- SRB Bedside ClinicDocument592 pagesSRB Bedside ClinicAbinesh Kumar100% (1)
- Paul Ekman Manual FACS Pages 352 357Document6 pagesPaul Ekman Manual FACS Pages 352 357LuisNo ratings yet
- Basic Lower Limb Assessment Flow SheetDocument2 pagesBasic Lower Limb Assessment Flow Sheetمحمد نعمة جياد100% (1)
- Skin TractionDocument10 pagesSkin Tractionpritinez2516100% (1)
- ProgramDocument11 pagesProgrammstephen244850% (2)
- 1.2.2.a SkeletonHunt 2016 - 17 No ConDocument4 pages1.2.2.a SkeletonHunt 2016 - 17 No ConjayNo ratings yet
- 02 - Fundamentals of OcclusionDocument22 pages02 - Fundamentals of OcclusionElena VasilescuNo ratings yet
- McNamara Analysis / Orthodontic Courses by Indian Dental AcademyDocument30 pagesMcNamara Analysis / Orthodontic Courses by Indian Dental Academyindian dental academy0% (1)
- Life Is Not an Accident: A Memoir of ReinventionFrom EverandLife Is Not an Accident: A Memoir of ReinventionRating: 3.5 out of 5 stars3.5/5 (7)
- Becky Lynch: The Man: Not Your Average Average GirlFrom EverandBecky Lynch: The Man: Not Your Average Average GirlRating: 4.5 out of 5 stars4.5/5 (13)
- Merle's Door: Lessons from a Freethinking DogFrom EverandMerle's Door: Lessons from a Freethinking DogRating: 4 out of 5 stars4/5 (326)
- Elevate and Dominate: 21 Ways to Win On and Off the FieldFrom EverandElevate and Dominate: 21 Ways to Win On and Off the FieldRating: 5 out of 5 stars5/5 (6)
- Welcome to the Goddamn Ice Cube: Chasing Fear and Finding Home in the Great White NorthFrom EverandWelcome to the Goddamn Ice Cube: Chasing Fear and Finding Home in the Great White NorthRating: 4 out of 5 stars4/5 (59)
- Crazy for the Storm: A Memoir of SurvivalFrom EverandCrazy for the Storm: A Memoir of SurvivalRating: 3.5 out of 5 stars3.5/5 (217)
- Survive!: Essential Skills and Tactics to Get You Out of Anywhere—AliveFrom EverandSurvive!: Essential Skills and Tactics to Get You Out of Anywhere—AliveNo ratings yet
- Bloodlines: The True Story of a Drug Cartel, the FBI, and the Battle for a Horse-Racing DynastyFrom EverandBloodlines: The True Story of a Drug Cartel, the FBI, and the Battle for a Horse-Racing DynastyRating: 4 out of 5 stars4/5 (8)
- House of Nails: A Memoir of Life on the EdgeFrom EverandHouse of Nails: A Memoir of Life on the EdgeRating: 3 out of 5 stars3/5 (4)
- What Winners Won't Tell You: Lessons from a Legendary DefenderFrom EverandWhat Winners Won't Tell You: Lessons from a Legendary DefenderRating: 4.5 out of 5 stars4.5/5 (7)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- Peak: The New Science of Athletic Performance That is Revolutionizing SportsFrom EverandPeak: The New Science of Athletic Performance That is Revolutionizing SportsRating: 5 out of 5 stars5/5 (96)
- The Perfect Mile: Three Athletes, One Goal, and Less Than Four Minutes to Achieve ItFrom EverandThe Perfect Mile: Three Athletes, One Goal, and Less Than Four Minutes to Achieve ItNo ratings yet
- The Rise of Superman: Decoding the Science of Ultimate Human PerformanceFrom EverandThe Rise of Superman: Decoding the Science of Ultimate Human PerformanceRating: 4.5 out of 5 stars4.5/5 (194)
- Badasses: The Legend of Snake, Foo, Dr. Death, and John Madden's Oakland RaidersFrom EverandBadasses: The Legend of Snake, Foo, Dr. Death, and John Madden's Oakland RaidersRating: 4 out of 5 stars4/5 (15)
- The Mindful Athlete: Secrets to Pure PerformanceFrom EverandThe Mindful Athlete: Secrets to Pure PerformanceRating: 4.5 out of 5 stars4.5/5 (278)
- The Last Dive: A Father and Son's Fatal Descent into the Ocean's DepthsFrom EverandThe Last Dive: A Father and Son's Fatal Descent into the Ocean's DepthsNo ratings yet
- Endure: How to Work Hard, Outlast, and Keep HammeringFrom EverandEndure: How to Work Hard, Outlast, and Keep HammeringRating: 4.5 out of 5 stars4.5/5 (285)
- Patriot Reign: Bill Belichick, the Coaches, and the Players Who Built a ChampionFrom EverandPatriot Reign: Bill Belichick, the Coaches, and the Players Who Built a ChampionRating: 3.5 out of 5 stars3.5/5 (30)
- Can't Nothing Bring Me Down: Chasing Myself in the Race Against TimeFrom EverandCan't Nothing Bring Me Down: Chasing Myself in the Race Against TimeRating: 4 out of 5 stars4/5 (1)
- Relentless: From Good to Great to UnstoppableFrom EverandRelentless: From Good to Great to UnstoppableRating: 5 out of 5 stars5/5 (784)
- How to Build a Car: The Autobiography of the World’s Greatest Formula 1 DesignerFrom EverandHow to Build a Car: The Autobiography of the World’s Greatest Formula 1 DesignerRating: 4.5 out of 5 stars4.5/5 (122)