Professional Documents
Culture Documents
Maternal The Lancet
Uploaded by
Hesty Kristianti PratiwiOriginal Description:
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Maternal The Lancet
Uploaded by
Hesty Kristianti PratiwiCopyright:
Available Formats
Series
Health in Southeast Asia 2
Maternal, neonatal, and child health in southeast Asia:
towards greater regional collaboration
Cecilia S Acuin, Geok Lin Khor, Tippawan Liabsuetrakul, Endang L Achadi, Thein Thein Htay, Rebecca Firestone, Zulfiqar A Bhutta
Although maternal and child mortality are on the decline in southeast Asia, there are still major disparities, and Published Online
greater equity is key to achieve the Millennium Development Goals. We used comparable cross-national data sources January 25, 2011
DOI:10.1016/S0140-
to document mortality trends from 1990 to 2008 and to assess major causes of maternal and child deaths. We present 6736(10)62049-1
inequalities in intervention coverage by two common measures of wealth quintiles and rural or urban status. Case
See Online/Comment
studies of reduction in mortality in Thailand and Indonesia indicate the varying extents of success and point to some DOI:10.1016/S0140-
factors that accelerate progress. We developed a Lives Saved Tool analysis for the region and for country subgroups to 6736(10)62192-7,
estimate deaths averted by cause and intervention. We identified three major patterns of maternal and child mortality DOI:10.1016/S0140-
6736(10)61426-2,
reduction: early, rapid downward trends (Brunei, Singapore, Malaysia, and Thailand); initially high declines (sustained
DOI:10.1016/S0140-
by Vietnam but faltering in the Philippines and Indonesia); and high initial rates with a downward trend (Laos, 6736(10)62143-5,
Cambodia, and Myanmar). Economic development seems to provide an important context that should be coupled DOI:10.1016/S0140-
with broader health-system interventions. Increasing coverage and consideration of the health-system context is 6736(10)62181-2,
DOI:10.1016/S0140-
needed, and regional support from the Association of Southeast Asian Nations can provide increased policy support
6736(10)61923-X, and
to achieve maternal, neonatal, and child health goals. DOI:10.1016/S0140-
6736(10)62140-X
Introduction This is the second in a Series of
Southeast Asia has achieved substantial reductions in Key messages six papers about health in
southeast Asia
child and maternal mortality over the past two decades, • Southeast Asia has sustained substantial reductions in Institute of Clinical
but these achievements are unevenly distributed among maternal, neonatal, and child mortality since 1990, but Epidemiology, University of
and within the countries in the region. Of the ten countries this progress has been uneven. Mortality reductions in the Philippines, National
in the Association of Southeast Asian Nations (ASEAN), some countries have been the result of trajectories of Institutes of Health, Ermita,
only three have infant and child mortality rates below ten rapid decline that started long before the Millennium
Manila, Philippines
(C S Acuin MD); Faculty of
per 1000 livebirths—Brunei, Singapore, and Malaysia. Development Goals (MDGs) were developed in 1990. Medicine and Health,
Infant and under-5 mortality in Thailand and Vietnam Others have succeeded in improving progress since the International Medical
have declined substantially to below 15 per 1000 livebirths 1990s, but some countries continue to struggle. University, Kuala Lumpur,
within the past two decades, but the Philippines and • Causes of death suggest a mortality transition in
Malaysia (Prof G L Khor PhD);
Epidemiology Unit, Faculty of
Indonesia have seen a levelling off in rates to between maternal deaths in the region. Child deaths are mainly Medicine, Prince of Songkla
30 and 50 per 1000 livebirths. Myanmar, Cambodia, and attributable to the persistence of neonatal causes along University, Hat Yai, Songkhla,
Laos still have mortality levels of 50–70 per 1000 livebirths with key preventable factors in the postneonatal period. Thailand (T Liabsuetrakul PhD);
in 2008, which are similar to the rates of their neighbours • Disparities in intervention coverage are most acute in
Faculty of Public Health,
University of Indonesia and
from more than two decades ago, and rank among the countries with the lowest intervention coverage overall. SEAMEO TROPMED, Regional
highest for Asia.1 • Despite the variations in achievements, some countries Center for Community
The UN estimates that every year about 350 000 women are notable success stories. Suggested key factors include Nutrition, Jakarta, Indonesia
die as a result of pregnancy or childbirth,2 as do nearly the ability to link maternal, neonatal, and child health
(E L Achadi DrPH); Public Health
Division, Department of
9 million children younger than 5 years.3 Worldwide, in interventions to broader health-system investments and Health, Ministry of Health,
2008, about 18 000 maternal2 and 400 000 child3 deaths to target access to rural and disadvantaged populations. Myanmar (T T Htay MD); China
were in southeast Asia. Laos and Cambodia are among • Increasing coverage to 60% will have a substantial effect on Medical Board , Cambridge,
seven countries with the highest maternal mortality ratios MA, USA (R Firestone ScD);
maternal deaths caused by unsafe abortion, hypertensive Harvard Global Equity
outside of sub-Saharan Africa, and Indonesia is one of 11 diseases, and postpartum haemorrhage and on neonatal Initiative, Boston, MA, USA
countries that account for 65% of all maternal deaths deaths caused by pneumonia, sepsis, and birth asphyxia. (R Firestone); and Department
worldwide.2 Although southeast Asia as a region might Although there might not be quick solutions for maternal, of Paediatrics and Child Health,
achieve the reductions in child mortality set by the UN Aga Khan University, Karachi,
neonatal, and child health in the region, coordinated Pakistan (Z A Bhutta PhD)
Millennium Development Goal 4 (MDG4), Cambodia and expansion of proven effective interventions can contribute Correspondence to:
Myanmar have been rated as having insufficient progress.4 to improved reductions in mortality. Dr Cecilia S Acuin, University of
Declines in mortality rates in Indonesia, Laos, and the • There is a need for stronger regional cooperation through the Philippines, National
Philippines are also faltering. Similarly, although all the Association of Southeast Asian Nations to provide Institutes of Health, Institute of
countries in the region are reporting declines in maternal Clinical Epidemiology, Pedro Gil,
support to countries that need to accelerate progress to Ermita, Manila 1000, Philippines
deaths (towards MDG5), the rates of decline for Indonesia, meet the MDGs. cesacuin@gmail.com
the Philippines, and Myanmar have notably slowed.
www.thelancet.com Published online January 25, 2011 DOI:10.1016/S0140-6736(10)62049-1 1
Series
national health problems. We first report on patterns of
Search strategy and selection criteria mortality reduction within southeast Asia and major
We searched the Demographic and Health Surveys (Cambodia 2000 and 2005; Indonesia causes of maternal and child deaths in the context of
1987, 1991, 1994, 2002–03, and 2007; Philippines 1993, 1998, 2003, and 2008; and MDG4 and MDG5. We investigate two country cases to
Vietnam 1997 and 2002),14 Multiple Indicators Cluster Surveys,15,16 data banks of regional highlight the notable variations in mortality reduction.
and global finance institutions such as the Asian Development Bank and the World Finally, we use an analysis of the deaths that could be
Bank,17–20,32 the Millennium Development Goals surveillance data sources4 and averted through expanded coverage to identify more
publications of the UN agencies, mainly UNICEF,3,15 and WHO1,2,40 from 1960 to October, effective approaches for improving maternal, neonatal,
2010. We used the following search terms: “Asia”, “Asia and Pacific”, “Southeast Asia”, and child health in southeast Asia.
“SEA”, “Association of Southeast Asian Nations”, and “ASEAN” (for geographic location);
“Cambodia”, “Indonesia”, “Lao PDR”, “Laos”, “Malaysia”, “Myanmar”, “Philippines”, Country-specific estimates on mortality rates
“Thailand”, and “Vietnam” (our countries of interest); “(maternal OR child OR neonatal) For the ten countries discussed in this paper, we reviewed
AND (health OR health care)”, “(health OR mortality) AND (pregnancy OR pregnant)”, estimates from national data sources and country
and “(health OR mortality) AND (maternal OR neonatal OR infant OR child OR under 5 Ministries of Health, as well as from the Demographic
years” (for health conditions); “health systems”, “health financing”, “leadership”, and Health Surveys and Multiple Indicator Cluster
“governance”, “information systems”, “delivery and organization of services”, “regulation Surveys. We also reviewed estimates from international
of health products”, “human resources” (for health systems); “maternal mortality ratio”, data sources from UNICEF, WHO, and the Institute for
“infant mortality rate”, “neonatal mortality rate”, “under 5 mortality rate”, “skilled birth Health Metrics and Evaluation (webappendix pp 1–2). We
attendance”, “antenatal care”, “prenatal care”, “immunization”, “maternal and child present country-specific estimates on maternal, neonatal,
nutrition”, and “causes of maternal, infant and child mortality” (for mortality and health and under-5 mortality rates from recent UN MDG
programme indicators); and “gross domestic product”, “GDP”, “GDP per capita”, “national reports,2,3 as these estimates enable cross-country
health accounts”, “NHA”, “public and private health expenditures”, and “(out-of-pocket comparisons on trends in mortality using replicable
OR OOP) health expenditures” (for finance). These data are complemented by nationally estimation methods that reduce sources of non-sampling
representative data and international journal publications. Specific country data were error. These estimates tend to be more conservative in
further verified and updated by members of the writing team. We also searched PubMed the rate of decline than estimates from the Institute for
from 1960 to October, 2010, for peer-reviewed journals for pertinent articles on Health Metrics and Evaluation. On the basis of increasing
maternal and child health and the region, and cross-referenced WHO, UNICEF, the World awareness of the burden of neonatal mortality, we sought
Bank, and the Asian Development Bank. No initial language exclusion was applied in comparable estimates of trends that separated neonatal
searching; for full-text papers, English and the languages of the authors (Thai, Bahasa, (death within the first 28 days after birth) and postneonatal
Malay, Chinese, Filipino, and Burmese) were used. (death between 28 days and 1 year after birth) mortality.
As UN models do not have neonatal time trends for all
countries in the region, we report estimates from the
See Online for webappendix Southeast Asia as a region has received little attention Institute for Health Metrics and Evaluation.11 We report
in recent efforts to revitalise and strengthen the policy estimates on causes of neonatal and child deaths on the
agenda of the Partnership for Maternal, Newborn and basis of standardised methods for estimating the
Child Health, despite the complexity of national trends, distribution of causes of child deaths.12 We compiled
including the substantial burden of morbidity and estimates of causes of maternal deaths from Countdown
mortality in several countries and the existence of 2015 country reports4 and WHO.13 We evaluated data
documented successes.5 As the economies of southeast from the Demographic and Health Surveys14 and Multiple
Asia become more integrated with each other, there is Indicator Cluster Surveys15,16 to assess existing intervention
an increasing need to assess and resolve the deficiencies coverage within the region, with these data sources
in this agenda and to identify policy options for providing the ability to disaggregate coverage estimates
sustaining, if not accelerating, the pace of reduction by wealth quintile and rural or urban status17–20 to establish
in mortality. the country average of coverage and to assess the
Effective and affordable technology to reduce most programme coverage in disadvantaged populations by
maternal, neonatal, and child deaths is available,6–9 so economic status and geography. We calculated regional
why has progress been so uneven? We focus on a estimates using country-level data from the specific
region, collectively the ninth largest economy in the source cited, unless otherwise indicated.
world, whose performance and achievements are often
hidden by larger countries such as India or China, as Analysis of the effect of interventions
well as by the UN agency groupings of the region that To test the contribution of health-sector inputs to
do not take into account historical and geopolitical ties mortality reductions, we selected Thailand and
within southeast Asia.10 In this paper, we critically Indonesia as case studies, as high (Thailand) and lower
review the region’s achievements in reducing maternal (Indonesia) achievers, and we focused on maternal and
and child mortality and highlight key factors that neonatal mortality as outcomes sensitive to health-
explain the successes and challenges in reaching these system development. We used national data for these
goals during competing worldwide, regional, and case studies to extend the analysis to the period before
2 www.thelancet.com Published online January 25, 2011 DOI:10.1016/S0140-6736(10)62049-1
Series
the MDG baseline year (1990).21,22 We fitted data to a
quadratic equation: A
1200 Malaysia
Thailand
log10MMR or log10NMR=Intercept+linear effect of year Philippines
+quadratic effect of year 1000 Indonesia
Maternal mortality (per 100 000 livebirths)
Vietnam
Laos
and to a linear equation: Cambodia
800 Myanmar
log10MMR or log10NMR=Intercept+linear effect of year
600
to establish whether declines in maternal mortality could
be attributed to programme changes or temporal trends, 400
where MMR is the maternal mortality ratio and NMR is
the neonatal mortality rate.
Using the Lives Saved Tool (LiST), we calculated 200
potential deaths that could be averted through increasing
population coverage of the interventions proven to be 0
effective in reducing maternal, neonatal, and child
mortality.23,24 LiST operates within the Spectrum B
modelling platform, by the Futures Group, initially 120
developed to project demographic change and
complemented by modules to model the effect of family
100
planning and HIV/AIDS interventions.25 The model
Infant mortality (per 1000 livebirths)
yields estimates of deaths averted by cause and
intervention for user-specified intervention coverage 80
levels, based on inputs of demographic projections,
numbers of maternal and child deaths, data on the 60
distribution of deaths by cause, intervention effectiveness,
and data on local health status.7,26–28 The platform has
40
been used previously for analysis of effect of intervention
packages on maternal and child survival in South Africa29
and sub-Saharan Africa,30 but this is one of the first uses 20
in southeast Asia. For this analysis, we assessed all the
maternal, neonatal, and child health interventions 0
included in LiST.31 The interventions and the estimates of
their effectiveness are provided in webappendix pp 3–8.
C
Values for the effectiveness of interventions were 160
developed through a standardised review process using
established criteria to identify which interventions to 140
include on the basis of levels of evidence.31 The analysis
Under-5 mortality (per 1000 livebirths)
was done for all ten countries and then for three 120
subgroups of countries on the basis of observed patterns
of mortality reduction: subgroup 1 (Brunei, Singapore, 100
Malaysia, Thailand); subgroup 2 (the Philippines,
80
Indonesia, Vietnam); and subgroup 3 (Laos, Cambodia,
Myanmar). We assessed potential lives saved at three 60
hypothetical coverage levels: 60%, 90%, and 99%.
40
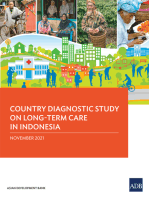
Patterns of mortality reduction
Reductions in maternal, infant, and child mortality in 20
southeast Asia are indicative of the diversity of this
0
region, presenting three divergent patterns (figure 1, data 1990 1995 2000 2005 2010
not shown for Brunei and Singapore as these countries Year
are considered to be more developed and where MDG
goals might not be as relevant).10,32 The first pattern Figure 1: Trends in maternal (A), infant (B), and under-5 (C) mortality in
reflects countries achieving low rates of mortality between southeast Asia (1990–2008)
1990 (the MDG baseline year) and 2008 in Brunei, Data from WHO2 (A) and UNICEF3 (B, C).
www.thelancet.com Published online January 25, 2011 DOI:10.1016/S0140-6736(10)62049-1 3
Series
Singapore, Malaysia, and Thailand. In 1990, maternal programme implementation and might not be as
mortality ratios in these countries were well below 100 per noticeably tracked towards their effect on under-5
100 000 livebirths, and infant and under-5 mortality rates mortality. The Philippines, which is deemed to be on
were already at or below 20 per 1000 livebirths. These target for MDG4 in achieving reductions in child
countries, the most economically advanced in the region, mortality,4 has the lowest reduction in neonatal mortality
have also invested in their health systems over time. in the region—lower than that for Cambodia or Myanmar,
A second, less distinct, pattern, seen in the Philippines, which have been identified as having insufficient progress
Indonesia, and Vietnam, starts with relatively high towards achieving MDG4.
mortality rates and ratios in 1990, fairly large initial
reductions (except for the maternal mortality ratio in Causes of mortality
Indonesia) that somewhat faltered after 2000 in Indonesia The distribution of maternal mortality causes (figure 2A)
and the Philippines. By contrast, there were accelerated is indicative of the substantial variations in health status
reductions in mortality in Vietnam during this period, and health-system development seen within the region.
with mortality rates and ratios beginning to come close Haemorrhage is a leading cause of death, probably
to those of Thailand. indicative of delays in attaining emergency obstetric care.
The third pattern, observed in Laos, Cambodia, and Hypertensive disorders contribute to about one in every
Myanmar has very high levels at the beginning of 1990, six maternal deaths in southeast Asia and suggest a
followed by sustained reductions from 1990 to 2005, with different causal pathway more similar to that in developed
the exception of Cambodia’s maternal mortality ratio.33 country settings. The proportion of other indirect causes
These three countries, which are on the UN list of least might indicate the still-substantial burden of infectious
developed countries, continue to report high rates of disease within the region and the effect of malaria and
maternal, infant, and child mortality. HIV on maternal health.33 Unsafe abortion is a factor in
Plotting maternal mortality reductions against gross almost 10% of maternal deaths. These patterns reflect a
national income per capita (webappendix p 9) indicates causal transition in maternal mortality as the overall risk
that, although countries with high maternal mortality of maternal death declines and these causes will affect the
achieved reductions in mortality as their gross national extent to which interventions, both as single modalities or
income per capita increased, some of the most notable included in a package, can be predicted to avert deaths.13
declines in mortality took place earlier than the rapid rise Different rates of reduction in child mortality can be
in gross national income. The rapid reductions in attributed partly to variations in causes of death
maternal mortality in Thailand occurred before 1990. As (figure 2B). Neonatal problems, such as preterm
maternal mortality declined to levels around 100, smaller complications, contributed to about 40% of child
reductions take place even as gross national income mortality, accounting for the single largest proportion of
continues to improve. Similar patterns are evident for preventable deaths, even as several ASEAN countries are
infant and under-5 mortality versus gross national successfully reducing their postneonatal and child
income per capita plots (webappendix pp 10–11). mortality burdens. Infectious diseases, including
pneumonia and diarrhoea, still account for almost half of
Neonatal and postneonatal mortality reductions the deaths in children, indicating substantial scope for
Separating infant mortality reduction between 1990 and continued reductions in child mortality.12
2010 into neonatal and postneonatal (webappendix p 12)
indicates that the largest declines in infant mortality Within-country disparities in intervention
over time were mainly attributable to substantial coverage
postneonatal mortality reductions, as seen in Malaysia, Inequalities are substantial across countries in the
Thailand, and Vietnam. The Philippines and Indonesia region, but also within countries, as indicated by the
had reductions in neonatal and postneonatal mortality current variation in intervention coverage by income
similar to that in Laos, Cambodia, and Myanmar. and by rural or urban subgroups (webappendix pp 13–15).
Although starting with comparably lower baseline Disparities exist in antenatal care coverage, use of skilled
mortality levels in 1990, rates of decline in the Philippines birth attendance, and diphtheria, polio, tetanus, and
and Indonesia were not sufficiently accelerated since the measles vaccination together with use of oral rehydration
development of the MDGs. Reductions in infant therapy, which are all key to the development of a
mortality in Brunei and Singapore stem from larger continuum of care.4,8
proportions of decline in neonatal deaths, a pattern With regard to overall programme coverage, Laos has a
similar to other high-income countries.34 substantially lower coverage than that of other countries
Other than Brunei and Singapore, the slower rates of in the region and is far from a 60% coverage level, even
decline for neonatal mortality for the other eight of the for the wealthier groups. Antenatal care coverage is the
ten ASEAN countries is a cause for concern. Interventions most widespread, being close to or above 90%, in
for reducing neonatal mortality are more closely linked countries other than Laos and Cambodia, for the
to maternal interventions in terms of policy and wealthier and urban areas. This disparity suggests that
4 www.thelancet.com Published online January 25, 2011 DOI:10.1016/S0140-6736(10)62049-1
Series
there is scope to effectively increase prenatal interventions
A
that can avert maternal deaths. Vaccination coverage Embolism 2%
varies widely between and within countries, although
several countries in the region are eligible for funds
from the Global Alliance for Vaccines and Immunisation
and have received substantial financial and policy
support that is likely to lead to increases in vaccination Sepsis
8%
coverage over time.
Laos and Cambodia have the greatest disparities in
programme coverage. In Cambodia, vaccination levels Hypertension
17% Haemorrhage
for the wealthiest quintile are similar to those of the other 32%
southeast Asia countries, matching those of Indonesia’s
highest quintile. However, the coverage in the poorest
households in Cambodia is almost 40% lower than that Abortion
for the wealthiest households, resulting in a large equity 9%
gap in immunisation levels. The countries shown in the
figures in webappendix pp 13–15 indicate relatively low Other
(direct) Other (indirect)
coverage of skilled birth attendance (except Thailand and 10% 22%
Vietnam) with inequality particularly acute in the
Philippines, Laos, and Cambodia. Differences in skilled
birth attendance between urban and rural Laotian
populations are the largest among the six countries
included in this comparison. Skilled birth attendance B
AIDS
could be viewed as one indicator of broader health-system 0·56%
development, and the generally low coverage coupled
with a high extent of inequality highlights the need for Malaria Measles
0·88% 0·46%
more comprehensive and coordinated health system
Meningitis Tetanus
improvements in the region overall.5 These patterns also 2·18% 0·44%
point to the necessity of targeting the most vulnerable Pertussis
Other non-communicable 0·32%
populations and maintaining attention to equity while diseases 3·77%
increasing programme coverage.35
Case studies: Thailand and Indonesia Preterm birth
To understand potential determinants of mortality complications
Injury 17·64%
reduction, we look in more depth at two countries with 8·35%
different experiences of lowering mortality. The reduction
in the maternal mortality in Thailand began in the 1960s
Neonatal causes
(webappendix p 16) at a time when skilled birth attendants, Diarrhoea of death
mostly midwives, were systematically trained and deployed 11·23% 38·97%
Birth asphyxia
to community hospitals.36–38 At the time of Alma-Ata in 9·83%
1978, Thailand’s maternal mortality ratio was already
below 200 and continued to drop even further in the 1980s
Other infections
as the economy improved and a health-care insurance 13·44%
programme for low-income populations was introduced Congenital
Pneumonia abnormalities
along with specific safe motherhood interventions. 19·42% 6·10%
Another round of health-system reforms and maternal,
neonatal, and child health interventions were introduced Neonatal sepsis
5·43%
in the early 2000s, including universal health coverage.
Coordinated health policy support through successive
national plans provided a context and investments to Figure 2: Causes of maternal (A) and child (B) deaths in southeast Asia
Data for maternal deaths are from UN MDG southeast Asia, 2010, including from ten ASEAN countries and Timor
stimulate structural, financial, and social capacities to
Leste (data not broken down to country level). Data for child deaths are from Black et al.12 ASEAN=Association of
deliver services, particularly in the district health Southeast Asian Nations.
system.21,39,40 Mandatory rural service for medical graduates
provided a stable human resource base within community and 1995, suggesting that the accelerated decline might
hospitals.36 be attributable to several developments. However, model
Using a log linear model, no single programme could fit after the 1997 economic crisis was not as good
explain the decline in maternal mortality between 1960 compared with earlier time periods. There was an
www.thelancet.com Published online January 25, 2011 DOI:10.1016/S0140-6736(10)62049-1 5
Series
increase in maternal mortality from 1997 to 2000,
A ASEAN region Regional subgroups followed by a steady decline. This decline was in parallel
Coverage levels 60% 90% 99% 60% 90% 99%
with economic recovery and the introduction of universal
Antepartum haemorrhage
Postpartum haemorrhage health insurance coverage, the provincial Maternal and
Hypertensive diseases Child Health Board groups, the Healthy Thailand
Sepsis infection programme, and the Saiyairak programme.21,39,40 For this
Abortion
Subgroup 1 short period, assessment of the effect of any intervention
Antepartum
haemorrhage
Subgroup 2 programmes is difficult.
Subgroup 3
Subgroup 1
The systematic deployment of community-based
Postpartum health personnel took place in Indonesia41 about a
Subgroup 2
haemorrhage
Subgroup 3 decade later than in Thailand in the 1970s. Major,
Subgroup 1
Hypertensive
Subgroup 2 targeted, safe motherhood initiatives were introduced in
diseases
Subgroup 3 the late 1980s, but by that time the maternal mortality
Subgroup 1
Sepsis
Subgroup 2
ratio of Indonesia was about nine times higher than that
infection of Thailand (webappendix pp 16–17).14,22 A village midwife
Subgroup 3
Subgroup 1 programme was implemented between 1989 and 1996,
Abortion Subgroup 2
Subgroup 3 but the comparatively rapid training and deployment of
54 000 village midwives might have compromised
B
quality of care.41
Diarrhoeal diseases
Access to care in Indonesia varies by rural or urban
Tetanus geography, income, and level of education. Unlike in
Pneumonia or sepsis Thailand, where the provision of skilled birth attendants
Preterm birth complications
Birth asphyxia was followed by increased facility and referral level
Diarrhoeal
Subgroup 1 capacities, in Indonesia not all health centres can provide
Subgroup 2 basic obstetric care. About 40% of district hospitals do
diseases
Subgroup 3
Subgroup 1 not have an obstetrician,41 indicating limited provision of
Tetanus Subgroup 2 the 24-h continuum of care necessary for dealing with
Subgroup 3
Subgroup 1
emergency situations. A fragmented and devolved health
Pneumonia system has challenged the capacity to sustain a
Subgroup 2
or sepsis
Subgroup 3 comprehensive and concerted focus on maternal and
Subgroup 1
Preterm birth
Subgroup 2 child health.
complications
Subgroup 3 Reductions in neonatal mortality (webappendix p 18)
Subgroup 1
Birth Subgroup 2
for the two countries mirror reductions in maternal
asphyxia Subgroup 3 mortality. Interventions to reduce neonatal mortality need
more from health systems than either a maternal or child
C programme alone.34 In Thailand, neonatal interventions
Diarrhoeal diseases have been linked with maternal programmes,36,39,40 but
Pneumonia this association has not been documented in Indonesia.
Measles
Meningitis
Maternal and neonatal mortality reductions in Thailand
Malaria and Indonesia occurred in the context of rapid economic
Subgroup 1 growth in both settings along with widespread increases
Diarrhoeal
Subgroup 2
diseases
Subgroup 3 in education levels and in sex equity.42 Although these
Subgroup 1 factors might have affected levels of success, other
Pneumonia Subgroup 2
Subgroup 3
determinants of mortality have been involved. Policy
Subgroup 1 implementation in Thailand has been multi-sectoral,
Measles Subgroup 2 involving royalty and different ministries, including the
Subgroup 3
Subgroup 1 National Health Security Office, which is responsible for
Meningitis Subgroup 2 health financing, especially universal coverage of health
Subgroup 3 insurance. Investments in primary health care in the
Subgroup 1
Malaria Subgroup 2 1970s have led to benefits in the long term.5 However,
Subgroup 3 geographic and demographic context also probably have a
0 20 40 60 80 100 role. At the time of its rapid maternal mortality reduction
Proportion of lives saved (%)
in the 1970s, Thailand had a smaller, more circumscribed
population compared with the larger and more dispersed
Figure 3: Maternal (A), neonatal (B), and child (C) deaths averted at 60, 90, and 99% coverage of
interventions for the ASEAN region and regional subgroups as defined by mortality reduction patterns
Indonesian population, and this difference might have
Subgroup 1=Brunei, Singapore, Malaysia, and Thailand; subgroup 2=the Philippines, Indonesia, and Vietnam; and been an important factor in establishing physical
subgroup 3=Laos, Cambodia, and Myanmar. ASEAN=Association of Southeast Asian Nations. access—a basic requirement for programme coverage.
6 www.thelancet.com Published online January 25, 2011 DOI:10.1016/S0140-6736(10)62049-1
Series
LiST analysis neonatal deaths in subgroup 3, whereas comprehensive
We investigated the potential effects of expanding obstetric care will save almost twice as many lives as basic
programme coverage through a LiST analysis of the care will for the region as a whole, but particularly for
ASEAN region as a whole, and for subgroups on the basis subgroups 2 and 3. However, even at 99% coverage the
of the mortality reduction patterns described earlier. We maximum proportion of neonates that could be saved
provide percentages rather than absolute numbers, as with either of these interventions does not go beyond a
these estimates should be interpreted with caution in the third of deaths, indicating the need for other interventions
context of local data. such as those that take into account prematurity through
The LiST analysis is under development as a measure antenatal steroids and providing Kangaroo care.48
for assessing and evaluating the benefits and limitations Interventions directed towards infectious diseases such
of interventions. Several of the interventions cited and as diarrhoea and pneumonia will, likewise, affect
used have been recently reviewed in depth25,43 and used for postneonatal and child deaths mostly in subgroups 2 and
regional estimates.44,45 These estimates are the best point 3. A small but noticeable effect on death in subgroup 1
estimates for the effect of interventions, and, although might also be apparent when coverage increases to 99%.
these have been validated against actual observed mortality Preventive measures such as improving access to safe
effects in the neonatal period,30 they still need prospective water can contribute substantially to mortality reduction,
validation for programme-based effectiveness. averting more deaths than would pneumococcal
ASEAN regional averages are closer to those of vaccination in all the subgroups.
subgroups 2 and 3 (as defined earlier), which consist of
the bulk of the population and the higher mortality rates Conclusions
(figure 3A). Although differences in maternal deaths Despite substantial improvements in maternal, neonatal,
averted across the groups are substantial, common trends and child health since 1990, most notably in Malaysia,
across the region highlight crucial gaps. Expanding Thailand, and Vietnam, high mortality, poor coverage,
coverage of interventions for hypertensive disease in and high inequity continue to challenge other countries
pregnancy and safe management of abortions, for
example, will reduce maternal deaths substantially Level of Subgroup 1 Subgroup 2 Subgroup 3 ASEAN region
throughout the region, and addressing postpartum evidence*
haemorrhage causes will largely reduce deaths for Maternal deaths averted (%)
subgroups 2 and 3 but not subgroup 1. Basic emergency obstetric Moderate 0·05 19·4 21·5 19·0
Counterpart calculations were made for neonatal and care (clinic)
child mortality (figure 3B and C). Interventions for birth Comprehensive emergency High 1·6 55·1 55·6 52·9
asphyxia are more likely to avert deaths in subgroups 2 and obstetric care
3 than in subgroup 1. The high proportion of neonatal and Basic postabortion case Moderate 8·8 5·8 5·8 5·9
management
child deaths averted through interventions for infectious
diseases in all subgroups is indicative that infectious Comprehensive postabortion High 12·1 6·5 6·5 6·7
case management
disease remains a challenge for the region as a whole.12,46
Neonatal deaths averted (%)
To focus on universal coverage, which is receiving
Basic emergency obstetric Moderate 0·03 11·7 17·2 12·8
greater attention in other health-policy settings,47 we care (clinic)
report the deaths that could be averted at 99% programme Comprehensive emergency Moderate 0·1 22·8 31·1 24·1
coverage. At the regional level, universal basic obstetric obstetric care
care coverage will save about one in five mothers (table), Antenatal corticosteroids for High 7·3 20·1 17·2 18·5
but with universal comprehensive obstetric care coverage, preterm labour
more than half of maternal deaths would be averted. Kangaroo care Moderate 20·3 20·6 16·8 19·4
Almost all these lives saved would be in subgroups 2 and Child (including postneonatal) deaths averted (%)
3 for which current levels of coverage for these services Use of safe water connection in Moderate 3·1 13·4 11·3 12·3
are low (webappendix pp 13–15). Because there is already the home
good access to basic and comprehensive obstetric care Pneumococcal vaccine High 2·9 9·8 7·6 8·7
for subgroup 1, the deaths averted from these Pneumonia case management High 5·7 19·0 15·9 17·4
(oral antibiotics)
interventions are minimal. By contrast, basic postabortion
Zinc for diarrhoea treatment High 1·2 5·0 3·9 4·4
case management will save a higher proportion of
mothers in subgroup 1 but more deaths will actually be Examples were selected for cases in which interventions might make the biggest differences and that indicate an
averted in subgroups 2 and 3. The fewer lives saved in approach to the use of LiST analysis. Level of evidence based on Grading of Recommendations Assessment,
Development and Evaluation (GRADE) assessment using the Child Health Epidemiology Reference Group (CHERG)
subgroup 1 with comprehensive abortion versus basic
methods.23,28 Subgroup 1=Brunei, Singapore, Malaysia, and Thailand; subgroup 2=the Philippines, Indonesia, and
abortion care might be because the access to Vietnam; and subgroup 3=Laos, Cambodia, and Myanmar. ASEAN=Association of Southeast Asian Nations.
comprehensive obstetric care that could be used for
Table: Percentage of deaths averted with 99% coverage of selected interventions for the ASEAN region
abortion management in this group is already high.
and for subgroups, as defined by mortality reduction patterns
Universal basic obstetric care will avert about one in five
www.thelancet.com Published online January 25, 2011 DOI:10.1016/S0140-6736(10)62049-1 7
Series
in the region, such as Laos, Cambodia, and Myanmar. methods; however, these estimates are preferred for
Improvements in the first three countries seem to be cross-country analysis. These estimates for southeast
attributable to socioeconomic progress and a consistent Asia are still mainly derived from household surveys and
policy focus on maternal and child health programmes subject to potential error from under-reporting and
and coordinated health-system components,49–51 notably a misclassification of deaths. Only five of the ten countries
stable and strategically deployed health workforce discussed have vital registration systems, and not all
coupled with supportive finance mechanisms in Malaysia these systems have valid registration of causes of death.2
and Thailand. The importance of favourable health There is an acute need for better data in Laos and
systems is highlighted by the case study in Thailand, Myanmar, particularly on maternal mortality, but the
which indicates that mortality reductions have taken pioneering work in maternal death audits in Malaysia
place at modest levels of economic growth and that no provides a potential model for the region.52
single factor or intervention could account for these The selection of data sources was mainly affected by
reductions. The case study in Indonesia indicates how the availability of comparable, reliable data across all the
similar interventions used in a setting with different ASEAN countries. For example, although we used the
system capacities and geopolitical features can result in more inclusive gross national income per capita for
different outcomes. webappendix pp 9–11, this measurement was not
Thus, although the LiST analysis can estimate the consistently available for the case studies, hence the use
potential effect of interventions given with maximum of gross domestic product for Thailand and Indonesia.
levels of coverage, the case studies caution us that We were not able to disaggregate LiST estimates into
improving health outcomes is not just about increasing relevant national subgroups by wealth or by rural or
the amount of money spent on health. Instead, targeted urban status. This non-separation is important because
and sustained interventions to reduce the barriers that the poor populations are likely to have higher mortality
prevent the most vulnerable population groups from rates and lower levels of intervention coverage than the
accessing the interventions they crucially need should be wealthier groups, which could affect estimates.43 Data
ensured in the long term. For example, the LiST analysis limitations restricted our ability to develop this analysis,
indicates that providing basic and comprehensive even as a test case. We have also not analysed the costs
emergency obstetric care has the potential to avert half of involved in extending coverage, which we hope to develop
all maternal deaths and about one in six neonatal deaths in a future study.
in Laos, Cambodia, and Myanmar. However, prevention Since its formation in 1967, ASEAN has positioned
of these deaths might be possible only if care coverage is itself as an important hub for economic and socio-
rapidly expanded in low-income and rural populations, cultural cooperation. Infectious diseases have thus far
possibly through sustained donor investments, given the commanded much of ASEAN’s attention in health
low levels of domestic health spending. In the Philippines matters. Recently, regional focus has begun to shift to
and Indonesia, the two most populous countries in the other health issues. The ASEAN Strategic Framework on
region, regaining momentum in mortality reduction Health Development 2010–2015,53 which focuses on
alongside substantial geographic and cultural access access to health-care services in addition to communicable
challenges might mean improving access to services diseases and pandemic preparedness, has also gained
through more equitable financing schemes.47 regional support.
Despite the varying agendas that countries of the region Given the economic vigour of ASEAN, regional
might need to adopt to complete the unfinished maternal, cooperation in health might be key to motivating less-
neonatal, and child health agenda, our findings indicate developed members to focus on maternal, neonatal,
important areas of common ground. Many key and child health. The pivotal role of ASEAN in
interventions to reduce child deaths have been stimulating and channelling international financial aid
implemented at the community level throughout to tsunami-devastated Indonesia in 2004 and cyclone-
southeast Asia, but necessary health-service investments stricken Myanmar in 2008 testifies to the power of this
that will enable the countries of the region to reduce promise—the goodwill and experience of working with
maternal and neonatal deaths have yet to be fully each other in disaster situations can be harnessed for
considered. Access to safe abortion services and the health and wellbeing of mothers and children in the
management of hypertensive disorders during pregnancy region.54,55
will prevent maternal deaths from these causes from But how should this aid be used? The experience of the
Brunei to Myanmar. Similarly, all countries in the region ASEAN, as discussed in this paper, suggests that effective
recognise space for expanding coverage of crucial interventions to curb maternal and child mortality need
neonatal interventions to prevent preterm births and to be deployed to actively target the disadvantaged
neonatal deaths from infection. populations who are most affected by unsafe abortion,
Our study has several limitations. We have used hypertensive diseases, postpartum haemorrhage,
estimates of mortality reduction from UN agencies that pneumonia, sepsis, and birth asphyxia. Far from
might not match national estimates and that use different expecting coverage of these programmes to passively
8 www.thelancet.com Published online January 25, 2011 DOI:10.1016/S0140-6736(10)62049-1
Series
diffuse to the very poor, governments must innovatively 4 Countdown to 2015. Maternal, Newborn and Child Health. 2010
combine health interventions with non-health country profiles. http://www.countdown2015mnch.org/reports-
publications/2010-country-profiles (accessed May 12, 2010).
programmes such as micro-finance schemes and 5 Rohde J, Cousens S, Chopra M, et al. 30 years after Alma-Ata:
conditional cash transfer mechanisms that have proven has primary health care worked in countries? Lancet 2008;
successful in other settings.56,57 372: 950–61.
6 Campbell OMR, Graham WJ, Lancet Maternal Survival Series
Achievement of the MDGs worldwide will not happen steering group. Strategies for reducing maternal mortality: getting
without individual country efforts. As the donor on with what works. Lancet 2006; 368: 1284–99.
community focuses its attention on the burdens of Africa 7 Darmstadt GL, Bhutta ZA, Cousens S, Adam T, Walker N,
de Bernis L, Lancet Neonatal Survival Steering Team. Evidence-
and south Asia, ASEAN countries must provide support based, cost-effective interventions: how many newborn babies can
to each other. Examples of such support mechanisms we save? Lancet 2005; 365: 977–88.
already in place include financial cooperation through 8 Kerber KJ, de Graft-Johnson JE, Bhutta ZA, Okong P, Starrs A,
the ASEAN surveillance process, which is an early Lawn JE. Continuum of care for maternal, newborn, and child
health: from slogan to service delivery. Lancet 2007; 370: 1358–69.
warning system to keep track of macroeconomic trends 9 Bhutta ZA, Ali S, Cousens S, et al. Interventions to address maternal,
and to provide early detection of any adverse development. newborn, and child survival: what difference can integrated primary
For public health, the ASEAN SARS Containment health care strategies make? Lancet 2008; 372: 972–89.
10 Chongsuvivatwong V, Phua KH, Yap MT, et al. Health and
Information Network exemplifies how member countries health-care systems in southeast Asia: diversity and transitions.
share essential information, best practices, and new Lancet 2011; published online Jan 25. DOI:10.1016/S0140-
findings for severe acute respiratory syndrome. However, 6736(10)61507-3.
11 Rajaratnam J, Marcus J, Flaxman A, et al. Neonatal, postnatal,
ASEAN has yet to develop initiatives for maternal, childhood, and under-5-mortality for 187 countries, 1970–2010:
neonatal, and child health, which could be developed a systematic analysis of progress towards Millennium Development
through sharing information and best practices (possibly Goal 4. Lancet 2010; 375: 1988–2007.
12 Black R, Cousens S, Johnson H, et al. Global, regional, and national
starting by resolving the absence of comparable data causes of child mortality in 2008: a systematic analysis. Lancet 2010;
across countries); financial cooperation efforts could be 375: 1969–87.
linked to outcomes, and the attainment of MDGs for 13 Khan KS, Wojdyla D, Say L, Gülmezoglu AM, Van Look PFA. WHO
member countries behind target could be made an analysis of causes of maternal death: a systematic review. Lancet
2006; 367: 1066–74.
ASEAN priority. 14 Measure DHS. Demographic and Health Surveys. http://www.
Contributors measuredhs.com (accessed April 27, 2010).
CSA, RF, GLK, TTH, TL, and EA contributed to the conception, design, 15 UNICEF. Multiple Indicator Cluster Surveys. UNICEF. http://www.
and acquisition of data for the first draft. TL, EA, and GLK contributed to childinfo.org/mics.html (accessed July 4, 2010).
the acquisition, analysis, and interpretation of data for the case studies. 16 National Statistics Office. Monitoring the situation of children and
ZB, RF, and CSA contributed to the acquisition, analysis, and women. Thailand multiple indicator cluster survey December
interpretation of data for the LiST analysis. CSA and RF were 2005–February 2006 Final Report. http://www.unicef.org/thailand/
responsible for the overall analysis and interpretation of data. All authors MICS_Final_Report2.pdf (accessed Sept 20, 2010).
contributed to the drafting and critical review of the paper. 17 Gwatkin D, Rutstein S, Johnson K, Suliman E, Wagstaff A,
Amouzou A. Socio-economic differences in health, nutrition, and
Conflicts of interest population in Cambodia. Washington, DC: The World Bank, 2007.
CSA is employed by the University of the Philippines, National Institutes 18 Gwatkin D, Rutstein S, Johnson K, Suliman E, Wagstaff A,
of Health and has received consultancy fees from projects with the Amouzou A. Socio-economic differences in health, nutrition, and
Philippine government, UNICEF, United States Agency for International population in Indonesia. Washington, DC: The World Bank, 2007.
Development, and WHO Regional Office for the Western Pacific. GLK 19 Gwatkin D, Rutstein S, Johnson K, Suliman E, Wagstaff A,
has received consultancy fees from the Institute of Gerontology, Amouzou A. Socio-economic differences in health, nutrition, and
Universiti Putra Malaysia, International Life Sciences Institute SEA, population in the Philippines. Washington, DC: The World Bank,
SEAMEO TROPMED Regional Centre for Community Nutrition, and is 2007.
employed by the International Medical University, Malaysia. All other 20 Gwatkin D, Rutstein S, Johnson K, Suliman E, Wagstaff A,
authors have no conflicts of interest. Amouzou A. Socio-economic differences in health, nutrition, and
population in Vietnam. Washington, DC: The World Bank, 2007.
Acknowledgments 21 Bureau of Policy and Strategy, Ministry of Public health. Thailand
This paper is part of a Series funded by the China Medical Board, Health Profile 2005–2007. Wibulpolprasert S, ed. Bangkok: The War
Rockefeller Foundation, and Atlantic Philanthropies. The authors thank Veterans Organization of Thailand Printing Press, 2007. http://
the following individuals for their assistance: Virasakdi www.moph.go.th/ops/thp/index.php?option=com_content&task=vi
Chongsuvivatwong, Edward McNeil (Epidemiology Unit, Faculty of ew&id=6&Itemid=2&lang=en (accessed Nov 22, 2010).
Medicine, Prince of Songkla University, Thailand), Marian Valera, 22 Ministry of Health, Indonesia. National Health Surveys 1980–2008.
Bryan Lim, Joan Javellana-Ottao (University of the Philippines, National Jakarta, Indonesia.
Institutes of Health), and Arjumand Rizvi (Aga Khan University, 23 Plosky WD, Stover J, Winfrey B. The Lives Saved Tool. A computer
Pakistan). program for making child and maternal survival projections.
UNICEF. 2009. http://www.jhsph.edu/bin/i/x/list_manual.pdf
References (accessed Nov 22, 2010).
1 WHO. World health statistics 2010. Geneva: World Health 24 Department of International Health. LiST: The Lives Saved Tool—
Organization, 2010. an evidence-based tool for estimating intervention impact. Johns
2 WHO. Trends in maternal mortality: 1990–2008. Geneva: World Hopkins University. http://www.jhsph.edu/dept/ih/IIP/list/index.
Health Organization, 2010. html (accessed Oct 30, 2010).
3 UNICEF. Levels and trends in child mortality, Report 2010. 25 Stover J, McKinnon R, Winfrey B. Spectrum: a model platform for
Estimates developed by the UN Inter-agency Group for Child linking impact of maternal and child survival intervention with
Mortality Estimation. United Nations Children’s Fund, 2010 http:// AIDS, family planning and demographic projections.
www.unicef.gr/pdfs/UNICEF_Levels_and_Trends_in_Child_ Int J Epidemiol 2010; 39 (suppl 1): i7–i10.
mortality.pdf (accessed Nov 22, 2010).
www.thelancet.com Published online January 25, 2011 DOI:10.1016/S0140-6736(10)62049-1 9
Series
26 Jones G, Steketee RW, Black RE, Bhutta ZA, Morris SS. The 42 Gakidou E, Cowling K, Lozano R, Murray CJL. Increased
Bellagio Child Survival Study Group. How many child deaths can educational attainment and its effects on child mortality in
we prevent this year? Lancet 2003; 362: 65–71. 175 countries between 1970 and 2009: a systematic analysis.
27 Bhutta ZA, Ahmad T, Black RE, et al, for the Maternal and Child Lancet 2010; 376: 959–74.
Undernutrition Study Group. What works? Interventions for 43 Victora CG. Commentary: LiST: using epidemiology to guide child
maternal and child undernutrition and survival. Lancet 2008; survival policymaking and programming. Int J Epidemiol 2010;
371: 417–40. 39 (suppl 1): i1–i2.
28 Boschi-Pinto C, Young M, Black RE. The child health epidemiology 44 Bryce J, Friberg I, Kraushaar D, et al. LiST as a catalyst in program
reference group reviews of the effectiveness of interventions to planning: experiences from Burkina Faso, Ghana and Malawi.
reduce maternal, neonatal and child mortality. Int J Epidemiol 2010; Int J Epidemiol 2010; 39 (suppl 1): i40–47.
39 (suppl 1): i3–i6. 45 Hazel E, Gilroy K, Friberg I, et al. Comparing modelled to measured
29 Chopra M, Daviaud E, Pattinson B, Fonn S, Lawn JE. Saving the mortality reductions: applying the Lives Saved Tool to evaluation
lives of South Africa’s mothers, babies, and children: can the health data from the Accelerated Child Survival Programme in
system deliver? Lancet 2009; 374: 835–46. West Africa. Int J Epidemiol 2010; 39 (suppl 1): i32–39.
30 Friberg IK, Kinney MV, Lawn JE, et al. Sub-Saharan Africa’s 46 Coker RJ, Hunter BM, Rudge JW, Liverani M, Hanvoravongchai P.
mothers, newborns, and children: how many lives could be saved Emerging infectious diseases in southeast Asia: regional challenges
with targeted health interventions? PLoS Med 2010; 7: e1000295. to control. Lancet 2011; published online Jan 25. DOI:10.1016/S0140-
31 Walker N, Fischer-Walker C, Bryce J, Bahl R, Cousens S,CHERG 6736(10)62004-1.
Review Groups on Intervention Effects. Standards for CHERG 47 Tangcharoensathien V, Patcharanarumol W, Ir P, et al.
reviews of intervention effects on child survival. Int J Epidemiol Health-financing reforms in southeast Asia: challenges in
2010; 39 (suppl 1): i21–i31. achieving universal coverage. Lancet 2011; published online Jan 25.
32 World Bank. World Development Indicators database. http:// DOI:10.1016/S0140-6736(10)61890-9.
siteresources.worldbank.org/DATASTATISTICS/Resources/ 48 Victora CG, Rubens CE, the GAPPS Review Group. Global report
GNIPC.pdf (accessed Sept 27, 2010). on preterm birth and stillbirth (4 of 7): delivery of interventions.
33 Hogan M, Foreman K, Naghavi M, et al. Maternal mortality for BMC Pregnancy Childbirth 2010; 10 (suppl 1): S4.
181 countries, 1980–2008: a systematic analysis of progress 49 Limwattananon S, Tangcharoensathien V, Prakongsai P. Equity in
towards Millennium Development Goal 5. Lancet 2010; maternal and child health in Thailand. Bull World Health Organ
375: 1609–23. 2010; 88: 420–27.
34 Lawn JE, Cousens S, Zupan J, Lancet Neonatal Survival Steering 50 UN Country Team Malaysia. Malaysia, Successes and challenges,
Team. 4 million neonatal deaths: When? Where? Why? Lancet 2005; Kuala Lumpur: United Nations Development Programme, 2005.
365: 891–900. http://www.undp.org.my/mdgs/malaysia-mdg-report (accessed
35 Boerma JT, Bryce J, Kinfu Y, Axelson H, Victora CG, Countdown Nov 22, 2010).
2008 Equity Analysis Group. Mind the gap: equity and trends in 51 Health Policy and Strategy Institute. Measuring health systems
coverage of maternal, newborn and child health services in performance in Vietnam: results from eight provincial health
54 Countdown countries. Lancet 2008; 371: 1259–67. systems assessments. http://www.healthsystems2020.org/content/
36 Wibulpolprasert S. Community financing: Thailand experience. resource/detail/2515/ (accessed Sept 25, 2010).
Health Policy Plan 1991; 6: 354–60. 52 Abu Bakar S, Mathews A, Jegasothy R, Ali R, Kandiah N. Strategy
37 Van Lerberghe W, De Brouwere V. Of blind alleys and things that for reducing maternal mortality. Bull World Health Organ 1999;
have worked: history’s lessons on reducing maternal mortality. 77: 190–93.
Studies Health Serve Organ Policy 2001; 17: 7–33. 53 Association of Southeast Asian Nations. Joint Statement of the
38 Bureau of Policy and Strategy, Ministry of Public Health. Health 10th ASEAN Health Ministers Meeting Singapore, 22 July 2010.
policy in Thailand. Nonthaburi: Ministry of Public Health, 2009. http://www.aseansec.org/24938.htm (accessed Oct 30, 2010).
http://bps.ops.moph.go.th/webenglish/Health%20Policy%209.pdf 54 ASEAN Regional Programme for Disaster Management. A regional
(accessed Nov 22, 2010). strategy for disaster reduction. http://www.aseansec.org/18455.htm
39 Pramualratana P, Wibulpolprasert S. Health insurance systems in (accessed Nov 22, 2010).
Thailand. Nonthaburi: Health System Research Institute, 2002. 55 Tripartite Core Group; the Government of the Union of Myanmar,
http://ihppthaigov.net/publication/attachbook/92/chapter3.pdf the United Nations, and the Association of Southeast Asian
(accessed Nov 22, 2010). Nations. Post-Nargis Joint Assessment (PONJA), July 2008. http://
40 WHO SEARO. Improving maternal, newborn and child health in www.aseansec.org/21765.pdf (accessed Nov 22, 2010).
the South-East Asia Region. Data source: Basic indicators: health 56 Ahmed MU, Islam SK, Quashem A, Ahmed N, CGAP Working
situation in south-east Asia, World Health Organization, South-East Group on Microinsurance. Health microinsurance: a comparative
Asia Region, 2004. study of three examples in Bangladesh. Good and Bad Practices
41 Azwar A. Evolution of safe-motherhood policies in Indonesia. 2005; case study 13.
Initiative for Maternal Mortality Programme Assessment 57 Fiszbein A, Schady N, Ferreira F, et al. Conditional cash transfers:
(IMMPACT), Country Co-ordinating Group & Technical Partners reducing present and future poverty. Washington, DC: The World
Meeting, Aberdeen, UK, January 2004. Bank, 2009.
10 www.thelancet.com Published online January 25, 2011 DOI:10.1016/S0140-6736(10)62049-1
You might also like
- Right Care 2: SeriesDocument9 pagesRight Care 2: SeriesVirgilioNo ratings yet
- PH MaternalDocument10 pagesPH MaternalCleoanne GallegosNo ratings yet
- School substitution program model decreases obesityDocument7 pagesSchool substitution program model decreases obesityPahang Reforansa PutraNo ratings yet
- Determinants of Stunting in inDocument3 pagesDeterminants of Stunting in inNur UfiyaNo ratings yet
- SSM - Population Health: ArticleDocument9 pagesSSM - Population Health: ArticledwiNo ratings yet
- SSM - Population Health: Muhammad Fikru Rizal, Eddy Van DoorslaerDocument10 pagesSSM - Population Health: Muhammad Fikru Rizal, Eddy Van DoorslaerRamadhan Dwi PrasetyoNo ratings yet
- Pathology and Laboratory Medicine in Low-Income and Middle-Income Countries 1Document12 pagesPathology and Laboratory Medicine in Low-Income and Middle-Income Countries 1Abraham DiazNo ratings yet
- Health in Southeast Asia 6: SeriesDocument11 pagesHealth in Southeast Asia 6: SeriesYantoNo ratings yet
- Community & Public Health NursingDocument13 pagesCommunity & Public Health NursingClarence ViboraNo ratings yet
- Py 16096Document9 pagesPy 16096neviNo ratings yet
- PIIS0140673616309461Document9 pagesPIIS0140673616309461Jose Angel BarreraNo ratings yet
- Regional Differences in Usage of Antenatal Care and Safe Delivery Services in Indonesia: Findings From A Nationally Representative SurveyDocument15 pagesRegional Differences in Usage of Antenatal Care and Safe Delivery Services in Indonesia: Findings From A Nationally Representative SurveyYeheskielNo ratings yet
- Maternal Health Care in India Access and Demand DeterminantsDocument21 pagesMaternal Health Care in India Access and Demand Determinantspat.medicinanatural Panapane NaturologiaNo ratings yet
- You Know You Are Sick Why Do You Carry A PregnancyDocument9 pagesYou Know You Are Sick Why Do You Carry A PregnancyadhiniNo ratings yet
- Effect of Nurse Therapeutic Communication On Patient Satisfaction in The Installation of Genreral Hospital in Massenrempulu, Enrekang DistrictDocument6 pagesEffect of Nurse Therapeutic Communication On Patient Satisfaction in The Installation of Genreral Hospital in Massenrempulu, Enrekang DistrictInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Modelling Number of Stunting Binominal RegressionDocument16 pagesModelling Number of Stunting Binominal RegressionFikran Ahmad Ahmad Al-HadiNo ratings yet
- The Biopsychosocial Determinants of Stun 6df91c01Document14 pagesThe Biopsychosocial Determinants of Stun 6df91c01Endang PitrianiNo ratings yet
- Aguirre PEA Et Al., 2019Document8 pagesAguirre PEA Et Al., 2019Estefania AyalaNo ratings yet
- Birth - 2021 - Fernandez Turienzo - A Realist Review To Explore How Midwifery Continuity of Care May Influence PretermDocument14 pagesBirth - 2021 - Fernandez Turienzo - A Realist Review To Explore How Midwifery Continuity of Care May Influence PretermUnmulNo ratings yet
- A Review of Child Stunting Determinants in IndonesiaDocument10 pagesA Review of Child Stunting Determinants in IndonesiaPutri SaripaneNo ratings yet
- Communication Rehabilitation in Sub-Saharan Africa: The Role of Speech and Language TherapistsDocument9 pagesCommunication Rehabilitation in Sub-Saharan Africa: The Role of Speech and Language TherapistsRachmawan WijayaNo ratings yet
- Promise, and Risks, of Conditional Cash Transfer Programmes: Richard Eastell, Jennifer S WalshDocument3 pagesPromise, and Risks, of Conditional Cash Transfer Programmes: Richard Eastell, Jennifer S WalshLester AteNo ratings yet
- 2020 State Wide Program To Reduce Preterm Birth WADocument18 pages2020 State Wide Program To Reduce Preterm Birth WAmadhuNo ratings yet
- Article 7 (W7)Document11 pagesArticle 7 (W7)ayaa222nbNo ratings yet
- Role of Career Advancement Practices OnDocument27 pagesRole of Career Advancement Practices OnfrankNo ratings yet
- Jurnal StuntingDocument17 pagesJurnal StuntingnatiyaNo ratings yet
- Analysis of Factors Affecting The Prevalence of Stunting On Children Under Five Years 8429Document11 pagesAnalysis of Factors Affecting The Prevalence of Stunting On Children Under Five Years 8429Demsa SimbolonNo ratings yet
- Stop StuntingDocument9 pagesStop StuntingID HansamuNo ratings yet
- Pi Is 0140673618316477Document28 pagesPi Is 0140673618316477VitaNo ratings yet
- Parent Article - PerthDocument9 pagesParent Article - PerthKriti ShuklaNo ratings yet
- Rumah Sehat Anti StuntingDocument13 pagesRumah Sehat Anti StuntingEdaNo ratings yet
- Rise of Chronic Diseases in Southeast Asia Calls for ActionDocument11 pagesRise of Chronic Diseases in Southeast Asia Calls for ActionDwi NopriyantoNo ratings yet
- 2614 ArticleText 14197 1 10 20201226Document10 pages2614 ArticleText 14197 1 10 20201226Cindy MangayaNo ratings yet
- Artificial Intelligence and Digital Health in GlobDocument12 pagesArtificial Intelligence and Digital Health in GlobInstalasi GiziNo ratings yet
- Factors Influencing Contraceptive Uptake Among Lactating Mothers (6-24 Months) - A Case Study of 2medical Reception Station (2MRS)Document7 pagesFactors Influencing Contraceptive Uptake Among Lactating Mothers (6-24 Months) - A Case Study of 2medical Reception Station (2MRS)NanaKarikariMintahNo ratings yet
- Journal Pone 0263751Document15 pagesJournal Pone 0263751Camilla NorazmanNo ratings yet
- The Correlation Between Health Beliefs A 58ba91c6Document9 pagesThe Correlation Between Health Beliefs A 58ba91c6Fauzia ZheptyaNo ratings yet
- Pone 0212847Document19 pagesPone 0212847christ_cruzerNo ratings yet
- Adoption of Mobile PHN Msgs On Delivery and Care of NewbornDocument13 pagesAdoption of Mobile PHN Msgs On Delivery and Care of NewbornMehedi HasanNo ratings yet
- Jurnal Indonesia 1Document11 pagesJurnal Indonesia 1Juli ArnithaNo ratings yet
- Children: Dental Caries and Oral Health in Children-Special IssueDocument3 pagesChildren: Dental Caries and Oral Health in Children-Special IssuecareNo ratings yet
- JSY EditDocument2 pagesJSY EditPrabir Kumar ChatterjeeNo ratings yet
- Current State of Stroke Care in The PhilippinesDocument7 pagesCurrent State of Stroke Care in The PhilippinesNur Raineer laden GuialalNo ratings yet
- Singaporepaper JOR 2011marchDocument9 pagesSingaporepaper JOR 2011marchAsh DenemNo ratings yet
- GlobalDocument12 pagesGlobalaisyahNo ratings yet
- Emerging Infectious Diseases in Southeast Asia: Regional Challenges To ControlDocument11 pagesEmerging Infectious Diseases in Southeast Asia: Regional Challenges To ControlAsyifa DelilaNo ratings yet
- Unmet Need and Its Reasons For Nonuse Contraceptive in East Java ProvinceDocument7 pagesUnmet Need and Its Reasons For Nonuse Contraceptive in East Java ProvinceDiyahHerowatiNo ratings yet
- Impact of Electronic Health Records in SDocument8 pagesImpact of Electronic Health Records in SSanchithya AriyawanshaNo ratings yet
- 2016 Article 473 PDFDocument11 pages2016 Article 473 PDFKathleen SorianoNo ratings yet
- Inequality in The Use of Maternal and Child Health Services in The Philippines: Do Pro-Poor Health Policies Result in More Equitable Use of Services?Document11 pagesInequality in The Use of Maternal and Child Health Services in The Philippines: Do Pro-Poor Health Policies Result in More Equitable Use of Services?Carrie Joy DecalanNo ratings yet
- Measuring Quality of Maternal and Newborn Care in Developing Countries Using Demographic and Health SurveysDocument20 pagesMeasuring Quality of Maternal and Newborn Care in Developing Countries Using Demographic and Health Surveysalifa9393No ratings yet
- Continuity of Maternal Healthcare Services UtilisaDocument11 pagesContinuity of Maternal Healthcare Services Utilisastevy ariskaNo ratings yet
- The Challenges in Philippine Health AgenDocument5 pagesThe Challenges in Philippine Health AgenKhristine GelNo ratings yet
- Making Pregnancy Safer Safer Pregnancy in Tamil NaduDocument100 pagesMaking Pregnancy Safer Safer Pregnancy in Tamil NaduUthayakumar KasthuriNo ratings yet
- Article 8 (W7)Document9 pagesArticle 8 (W7)ayaa222nbNo ratings yet
- Relationship Between Equipment Availability With Health Services Integrated Elderly Service Post in Indonesia: Cross Sectional StudyDocument4 pagesRelationship Between Equipment Availability With Health Services Integrated Elderly Service Post in Indonesia: Cross Sectional StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Effectiveness of The Father Alert Android Application On Father's Knowledge and Support in Stunting Prevention in 2023Document6 pagesEffectiveness of The Father Alert Android Application On Father's Knowledge and Support in Stunting Prevention in 2023International Journal of Innovative Science and Research TechnologyNo ratings yet
- 01-Facilitators and Barriers For The Delivery and Uptake of Cervical Cancer Screening in IndonesiDocument16 pages01-Facilitators and Barriers For The Delivery and Uptake of Cervical Cancer Screening in IndonesiInggita Adinda PutriNo ratings yet
- Maternal Knowledge, Attitudes and Practices Towards Prevention and Management of Child Diarrhoea in Urban and Rural Maseru, LesothoDocument20 pagesMaternal Knowledge, Attitudes and Practices Towards Prevention and Management of Child Diarrhoea in Urban and Rural Maseru, LesothoAnisa SafutriNo ratings yet
- Incubating Indonesia’s Young Entrepreneurs:: Recommendations for Improving Development ProgramsFrom EverandIncubating Indonesia’s Young Entrepreneurs:: Recommendations for Improving Development ProgramsNo ratings yet
- 950215man 06187Document58 pages950215man 06187Electrònica Mèdica De La LagunaNo ratings yet
- Nursing Comps Study GuideDocument15 pagesNursing Comps Study GuideforminskoNo ratings yet
- Jamnagar Thesis 2004Document12 pagesJamnagar Thesis 2004Swagath NNo ratings yet
- Diagnostic Report SummaryDocument5 pagesDiagnostic Report SummaryShalini Rakesh JunejaNo ratings yet
- Resume 2019Document1 pageResume 2019api-316723361No ratings yet
- Bio OssDocument4 pagesBio OssVizi AdrianNo ratings yet
- YamamotoDocument11 pagesYamamotolopezhectora100% (1)
- Caesalpinia CristaDocument5 pagesCaesalpinia CristaDarmawan Said100% (1)
- Class 11 English Snapshots Chapter 7Document2 pagesClass 11 English Snapshots Chapter 7Alpha StarNo ratings yet
- PhobiasDocument10 pagesPhobiasapi-276690632No ratings yet
- Sage Char-Lee ResumeDocument2 pagesSage Char-Lee Resumeapi-510197139No ratings yet
- Bioequivalence Comparison Between Two Different Formulations of Alverine AriqDocument5 pagesBioequivalence Comparison Between Two Different Formulations of Alverine AriqHendri WijayaNo ratings yet
- Ifu Somatom DriveDocument600 pagesIfu Somatom DriveImc Muati100% (1)
- Anvisa National Health Surveillance AgencyDocument52 pagesAnvisa National Health Surveillance AgencyVimarsha HSNo ratings yet
- Evaluation of scales in immune-mediated polyneuropathiesDocument222 pagesEvaluation of scales in immune-mediated polyneuropathiesAngelo MalerbaNo ratings yet
- HypothyroidismfinalpptDocument91 pagesHypothyroidismfinalpptswathi bsNo ratings yet
- This Just In!: Queen Pin Carla!Document10 pagesThis Just In!: Queen Pin Carla!BS Central, Inc. "The Buzz"No ratings yet
- The Divine Message of Yog Rishi.: Swastha Ho Jan, Gan, Man and The Nation 'Document68 pagesThe Divine Message of Yog Rishi.: Swastha Ho Jan, Gan, Man and The Nation 'Aniket ShahNo ratings yet
- Bilirubin Production: Hemoglobin (70 To 80%) Erythroid Cells Heme Proteins Myoglobin, Cytochromes (20 To 25%)Document5 pagesBilirubin Production: Hemoglobin (70 To 80%) Erythroid Cells Heme Proteins Myoglobin, Cytochromes (20 To 25%)Daffa Samudera Nakz DoeratipNo ratings yet
- Pulmonary EmbolismDocument93 pagesPulmonary EmbolismRakesh PanchalNo ratings yet
- HIMSS EMRAM Stage 7 DMTDocument20 pagesHIMSS EMRAM Stage 7 DMTclrhoadesNo ratings yet
- Clinical Experience With The Constellation Vision SystemDocument16 pagesClinical Experience With The Constellation Vision SystemMohammad Abdullah BawtagNo ratings yet
- Hybrid Hyrax Distalizer JO PDFDocument7 pagesHybrid Hyrax Distalizer JO PDFCaTy ZamNo ratings yet
- DAFTAR OBAT LASA (Look Alike Sound AlikeDocument4 pagesDAFTAR OBAT LASA (Look Alike Sound Aliketri tanayawatiNo ratings yet
- Akupuntur 7Document9 pagesAkupuntur 7Ratrika SariNo ratings yet
- CBT IdDocument14 pagesCBT IdNASC8No ratings yet
- Influence of The Quality of The FinishedDocument6 pagesInfluence of The Quality of The Finishedmehdi chahrourNo ratings yet
- Novo NordiskDocument2 pagesNovo NordiskSpotlightNo ratings yet
- Birth Plan + Hospital Bag Checklist: The Best EverDocument32 pagesBirth Plan + Hospital Bag Checklist: The Best Everelly fadhliahNo ratings yet
- Review of Literature: MorphologyDocument38 pagesReview of Literature: MorphologyVaishu Gunalan0% (1)