You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- STIHL TS410, TS420 Spare PartsDocument11 pagesSTIHL TS410, TS420 Spare PartsMarinko PetrovićNo ratings yet
- Zanussi Parts & Accessories - Search Results3 - 91189203300Document4 pagesZanussi Parts & Accessories - Search Results3 - 91189203300Melissa WilliamsNo ratings yet
- Family Planning MethodsDocument20 pagesFamily Planning MethodsRoel Marcial100% (2)
- Major Chnage at Tata TeaDocument36 pagesMajor Chnage at Tata Teasheetaltandon100% (1)
- Montessori Vs WaldorfDocument4 pagesMontessori Vs WaldorfAbarnaNo ratings yet
- Functions of The Gastrointestinal Organs: Muhammad ImranDocument21 pagesFunctions of The Gastrointestinal Organs: Muhammad ImranSalman KhanNo ratings yet
- PNP Loan Application Form February 2021 16Document6 pagesPNP Loan Application Form February 2021 16Wilhelm RegaladoNo ratings yet
- Outbound Idocs Code Error Event Severity Sap MeaningDocument2 pagesOutbound Idocs Code Error Event Severity Sap MeaningSummit YerawarNo ratings yet
- ARMY - Chapter Eight Explosive BreachingDocument25 pagesARMY - Chapter Eight Explosive Breachingrsreeth100% (1)
- Instruction Manual Il-Obct-R1: Slip-Over Current Transformer ObctDocument2 pagesInstruction Manual Il-Obct-R1: Slip-Over Current Transformer Obctبوحميدة كمالNo ratings yet
- Design of Ka-Band Low Noise Amplifier Using CMOS TechnologyDocument6 pagesDesign of Ka-Band Low Noise Amplifier Using CMOS TechnologyEditor IJRITCCNo ratings yet
- The Eye WorksheetDocument3 pagesThe Eye WorksheetCally ChewNo ratings yet
- VRealize Operations Manager Installation and Configuration Guide For Linux and WindowsDocument98 pagesVRealize Operations Manager Installation and Configuration Guide For Linux and Windowsamdusias67No ratings yet
- Objective-C Succinctly PDFDocument110 pagesObjective-C Succinctly PDFTKKNo ratings yet
- Case Study On "Unilever in Brazil-Marketing Strategies For Low Income Consumers "Document15 pagesCase Study On "Unilever in Brazil-Marketing Strategies For Low Income Consumers "Deepak BajpaiNo ratings yet
- Interventional Studies 2Document28 pagesInterventional Studies 2Abdul RazzakNo ratings yet
- COE301 Lab 2 Introduction MIPS AssemblyDocument7 pagesCOE301 Lab 2 Introduction MIPS AssemblyItz Sami UddinNo ratings yet
- Chapter 4 PDFDocument26 pagesChapter 4 PDFMeloy ApiladoNo ratings yet
- You'Re My Everything - Glenn FredlyDocument2 pagesYou'Re My Everything - Glenn FredlyTommy Juliansyah MarsenoNo ratings yet
- LUNG ARTIFACTSreviewDocument13 pagesLUNG ARTIFACTSreviewMayra ValderramaNo ratings yet
- Practical Research 2 Group 11 RRL, Proposed Title and Answers To The QuestionsDocument14 pagesPractical Research 2 Group 11 RRL, Proposed Title and Answers To The QuestionsFeby Margaret AngNo ratings yet
- Procedure Manual - IMS: Locomotive Workshop, Northern Railway, LucknowDocument8 pagesProcedure Manual - IMS: Locomotive Workshop, Northern Railway, LucknowMarjorie Dulay Dumol80% (5)
- The Uv Environment Production System Best Practice OperationDocument2 pagesThe Uv Environment Production System Best Practice OperationFarzad ValizadehNo ratings yet
- Chapter5A TorqueDocument32 pagesChapter5A TorqueShuq Faqat al-FansuriNo ratings yet
- Title - Dating Virtual To Coffee Table Keywords - Dating, Application BlogDocument3 pagesTitle - Dating Virtual To Coffee Table Keywords - Dating, Application BlogRajni DhimanNo ratings yet
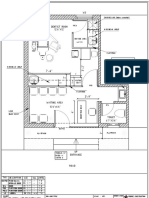
- Dental Clinic - Floor Plan R3-2Document1 pageDental Clinic - Floor Plan R3-2kanagarajodisha100% (1)
- Statistics and Probability Course Syllabus (2023) - SignedDocument3 pagesStatistics and Probability Course Syllabus (2023) - SignedDarence Fujihoshi De AngelNo ratings yet
- Porsche Dealer Application DataDocument3 pagesPorsche Dealer Application DataEdwin UcheNo ratings yet
- PCZ 1503020 CeDocument73 pagesPCZ 1503020 Cedanielradu27No ratings yet
- Synopsis SsDocument14 pagesSynopsis SsJYOTI KATIYAR SVUNo ratings yet