You might also like
- Benign and Pathological Chromosomal Imbalances: Microscopic and Submicroscopic Copy Number Variations (CNVs) in Genetics and CounselingFrom EverandBenign and Pathological Chromosomal Imbalances: Microscopic and Submicroscopic Copy Number Variations (CNVs) in Genetics and CounselingNo ratings yet
- DR Preeti Mansukhani - CBC 5 Parts - 2017Document56 pagesDR Preeti Mansukhani - CBC 5 Parts - 2017Silence T-jmNo ratings yet
- Interferences in Platelet: CountingDocument5 pagesInterferences in Platelet: CountingIberisNo ratings yet
- 09 Platelet Count by Peripheral Smear and Automated Cell Counter PDFDocument4 pages09 Platelet Count by Peripheral Smear and Automated Cell Counter PDFanggaririnNo ratings yet
- Citometria 2005Document8 pagesCitometria 2005Leslie AraujoNo ratings yet
- Etiological Potential of Immature Platelet Fraction in Children With ThrombocytopeniaDocument29 pagesEtiological Potential of Immature Platelet Fraction in Children With Thrombocytopeniajhanavi rajeshNo ratings yet
- Briggs 2009Document13 pagesBriggs 2009anggaririnNo ratings yet
- Platelet CountsDocument35 pagesPlatelet Countsshikhar623No ratings yet
- DocumentjkDocument6 pagesDocumentjksheilaNo ratings yet
- Dr. Yusra Rashid Haematology Department University of Health SciencesDocument40 pagesDr. Yusra Rashid Haematology Department University of Health SciencesMahmood AtharNo ratings yet
- Accurasi Perhitungan PlateletDocument68 pagesAccurasi Perhitungan PlateletMaria Yosefina HeraNo ratings yet
- Automated Counters3Document14 pagesAutomated Counters3Jacky SharmaNo ratings yet
- Novel Automated Hematology Parameters in Clinical Pediatric PracticeDocument9 pagesNovel Automated Hematology Parameters in Clinical Pediatric PracticerahulNo ratings yet
- Advances in Platelet CountingDocument8 pagesAdvances in Platelet CountingKamran DawoodNo ratings yet
- How I DiagnoseDocument17 pagesHow I DiagnoseFa FeNo ratings yet
- Bruegel 2015Document15 pagesBruegel 2015my accountNo ratings yet
- New QuantitiesDocument6 pagesNew Quantities20100117 Bùi Thùy VyNo ratings yet
- Lab Activity No. 8 - Slide PresentationDocument20 pagesLab Activity No. 8 - Slide PresentationChelsea Padilla Delos ReyesNo ratings yet
- Platelet Counting by The Coulter LH 750, Sysmex XE 2100Document7 pagesPlatelet Counting by The Coulter LH 750, Sysmex XE 2100blanket_thNo ratings yet
- Ajcpath126 0691Document8 pagesAjcpath126 0691sishui uchihaNo ratings yet
- Bone Marrow Evaluation of Patients Having Pancytopenia at Tertiary Care Center, M. Y. Hospital, Indore, India: One-Year StudyDocument4 pagesBone Marrow Evaluation of Patients Having Pancytopenia at Tertiary Care Center, M. Y. Hospital, Indore, India: One-Year StudyivanNo ratings yet
- 2 Ijmpsapr20172Document6 pages2 Ijmpsapr20172TJPRC PublicationsNo ratings yet
- Buttarello-2016-International Journal of Laboratory HematologyDocument10 pagesButtarello-2016-International Journal of Laboratory HematologyLaurentiusJohanNo ratings yet
- "Normal" Mean Corpuscular Volume Does Not Exclude The Diagnosis of ThalassaemiaDocument3 pages"Normal" Mean Corpuscular Volume Does Not Exclude The Diagnosis of ThalassaemiaTanveerNo ratings yet
- 3 Wood Flow HematopoieticDocument24 pages3 Wood Flow Hematopoieticalper togayNo ratings yet
- Correlation of Platelet Count With Variceal Hemorrhage During Ligation in Hepatic Cirrhosis PatientsDocument4 pagesCorrelation of Platelet Count With Variceal Hemorrhage During Ligation in Hepatic Cirrhosis PatientsMasriyaniNo ratings yet
- Hematology 1 (Laboratory) - Week 10-11 ModuleDocument8 pagesHematology 1 (Laboratory) - Week 10-11 ModuleJam RamosNo ratings yet
- Sysmex SEED Platelet Detection and The Importance of A Reliable CountDocument7 pagesSysmex SEED Platelet Detection and The Importance of A Reliable CountMuhammad Khoirut TNo ratings yet
- Group 6 Hema2 Exp 2Document3 pagesGroup 6 Hema2 Exp 2Aaron Tzergio GotohNo ratings yet
- Utility - of - Scatterplot - Patterns - of - Automated - Hematology Analysers 2020Document6 pagesUtility - of - Scatterplot - Patterns - of - Automated - Hematology Analysers 2020tufis02No ratings yet
- Using Hematology Instrument Data To TroubleshootDocument82 pagesUsing Hematology Instrument Data To Troubleshootuber6791No ratings yet
- Clinical SS - 2015 Kanter - BMC MedDocument8 pagesClinical SS - 2015 Kanter - BMC MedJoseAngelBarreraAlvarezNo ratings yet
- Labmed40 0227Document5 pagesLabmed40 0227Airell Takinan DumangengNo ratings yet
- Anemia Diagnosis, Classification, and Monitoring Using Cell-Dyn Technology Reviewed For The New MillenniumDocument16 pagesAnemia Diagnosis, Classification, and Monitoring Using Cell-Dyn Technology Reviewed For The New MillenniumNeveen_Hussein_1880No ratings yet
- Science: Assessment of The Reliability of The Sysmex XE-5000 Analyzer To Detect Platelet ClumpsDocument6 pagesScience: Assessment of The Reliability of The Sysmex XE-5000 Analyzer To Detect Platelet ClumpsnivmastNo ratings yet
- Guide: Dr. (MRS.) Jadhav M. VDocument92 pagesGuide: Dr. (MRS.) Jadhav M. VVivek PatelNo ratings yet
- Platelet Estimation by Manual and AutomationDocument4 pagesPlatelet Estimation by Manual and AutomationKamran DawoodNo ratings yet
- Digital Microscopy As A Screening Tool For The Diagnosis of Hereditary Hemolytic AnemiaDocument10 pagesDigital Microscopy As A Screening Tool For The Diagnosis of Hereditary Hemolytic AnemiaRanhie Pen'ned CendhirhieNo ratings yet
- Hem Lab Microhematocrit F15Document10 pagesHem Lab Microhematocrit F15Joan Christie WijayaNo ratings yet
- Sedimento RBC DismorficCellDocument7 pagesSedimento RBC DismorficCellecko RomanNo ratings yet
- Null 1Document49 pagesNull 1ImamAbdyNo ratings yet
- 4-Hematology Analyzer - Detecting Erroneous Blood CountsDocument23 pages4-Hematology Analyzer - Detecting Erroneous Blood CountsRajeshNo ratings yet
- Ok 2Document7 pagesOk 2cydolusNo ratings yet
- Rodak's Hematology 6th Edition Test BankDocument255 pagesRodak's Hematology 6th Edition Test Bankromerolourdes4No ratings yet
- Full Blood Count Apr04, DR Eva RaikDocument7 pagesFull Blood Count Apr04, DR Eva RaikDanielcc LeeNo ratings yet
- Int J Lab Hematology - 2022 - Marinov - Validation of A Single Tube 3 Colour Immature Red Blood Cell Screening Assay ForDocument7 pagesInt J Lab Hematology - 2022 - Marinov - Validation of A Single Tube 3 Colour Immature Red Blood Cell Screening Assay ForMaria SousaNo ratings yet
- Automation in Haematology 5-1Document50 pagesAutomation in Haematology 5-1Raphael AnajeNo ratings yet
- HemaDocument59 pagesHemaSteph VeeNo ratings yet
- Dimal HemaDocument8 pagesDimal HemaGioAndrew ReyesNo ratings yet
- Stefanini 1999Document5 pagesStefanini 1999Igor DemićNo ratings yet
- Evaluation of The Performance of The Sysmex XT-200Document11 pagesEvaluation of The Performance of The Sysmex XT-200Игорь БеняNo ratings yet
- Erroneous Automated Optical Platelet Counts PDFDocument8 pagesErroneous Automated Optical Platelet Counts PDFfar faraNo ratings yet
- A Manual of Laboratory Techniques in Clinical Hematology 1Document15 pagesA Manual of Laboratory Techniques in Clinical Hematology 1Jaycel Mae Ba-ay (Gaikokujinn)No ratings yet
- Hema I Chapter 8 - DiffDocument67 pagesHema I Chapter 8 - DiffderibewNo ratings yet
- Hematology 1 Lab - The Reticulocyte CountDocument17 pagesHematology 1 Lab - The Reticulocyte CountCIRILO MABBORANGNo ratings yet
- Hemat Cases ARUP Webinar 2015 - Compressed2new PDFDocument53 pagesHemat Cases ARUP Webinar 2015 - Compressed2new PDFDenise CssNo ratings yet
- Mean Platelet Volume, Platelet Distribution WidthDocument7 pagesMean Platelet Volume, Platelet Distribution WidthMarcellia AngelinaNo ratings yet
- Investigation of Platelet Function in Patients With Chronic Kidney Disease Stages IV-VDocument16 pagesInvestigation of Platelet Function in Patients With Chronic Kidney Disease Stages IV-VFrany CharismaNo ratings yet
- Automated Hematology Cell CountersDocument53 pagesAutomated Hematology Cell CountersFidaa Jaafrah100% (2)
- FBC Analysers and FBC InterpretationDocument63 pagesFBC Analysers and FBC InterpretationNikkole PhalulaNo ratings yet
- Donor S Tax Exam AnswersDocument6 pagesDonor S Tax Exam AnswersAngela Miles DizonNo ratings yet
- (Durt, - Christoph - Fuchs, - Thomas - Tewes, - Christian) Embodiment, Enaction, and Culture PDFDocument451 pages(Durt, - Christoph - Fuchs, - Thomas - Tewes, - Christian) Embodiment, Enaction, and Culture PDFnlf2205100% (3)
- Visual Rhetoric Music Video Comparison Essay - Abby MckellopDocument5 pagesVisual Rhetoric Music Video Comparison Essay - Abby Mckellopapi-597591424No ratings yet
- Flow ChemistryDocument6 pagesFlow Chemistryrr1819No ratings yet
- Gothic Revival ArchitectureDocument19 pagesGothic Revival ArchitectureAlexandra Maria NeaguNo ratings yet
- CURRICULUM VITAE Kham Khan Suan Hausing, PHDDocument8 pagesCURRICULUM VITAE Kham Khan Suan Hausing, PHDCinpu ZomiNo ratings yet
- Mathematics in The Primary Curriculum: Uncorrected Proof - For Lecturer Review OnlyDocument12 pagesMathematics in The Primary Curriculum: Uncorrected Proof - For Lecturer Review OnlyYekeen Luqman LanreNo ratings yet
- Habanera Botolena & Carinosa (Gas-A)Document8 pagesHabanera Botolena & Carinosa (Gas-A)christian100% (4)
- The Role of Financial System in DevelopmentDocument5 pagesThe Role of Financial System in DevelopmentCritical ThinkerNo ratings yet
- Individual Psychology (Adler)Document7 pagesIndividual Psychology (Adler)manilyn dacoNo ratings yet
- FreeMarkets: Procurement & Outsourcing StrategiesDocument44 pagesFreeMarkets: Procurement & Outsourcing StrategiesFarhaad MohsinNo ratings yet
- Clothing, Personality and Impressions PDFDocument11 pagesClothing, Personality and Impressions PDFAhmad RaoNo ratings yet
- Assignment Submission Form: Pgid Name of The MemberDocument9 pagesAssignment Submission Form: Pgid Name of The MemberNamit GaurNo ratings yet
- Osteoporosis: Prepared By: Md. Giash Uddin Lecturer, Dept. of Pharmacy University of ChittagongDocument30 pagesOsteoporosis: Prepared By: Md. Giash Uddin Lecturer, Dept. of Pharmacy University of Chittagongsamiul bashirNo ratings yet
- ATLS Note Ed 10Document51 pagesATLS Note Ed 10Nikko Caesario Mauldy Susilo100% (10)
- LET Facilitating Learning EDITED3Document12 pagesLET Facilitating Learning EDITED3Likhaan PerformingArts HomeStudio100% (5)
- MTAP Math ChallengeDocument5 pagesMTAP Math ChallengeHaron Abedin100% (1)
- Darkness Points Reminder 2Document2 pagesDarkness Points Reminder 2Tata YoyoNo ratings yet
- BSCHMCTT 101Document308 pagesBSCHMCTT 101JITTUNo ratings yet
- Measures-English, Metric, and Equivalents PDFDocument1 pageMeasures-English, Metric, and Equivalents PDFluz adolfoNo ratings yet
- Marketing Plan For Paraiso Islet ResortDocument25 pagesMarketing Plan For Paraiso Islet ResortEllaine Claire Lor100% (1)
- Final Research ReportDocument14 pagesFinal Research ReportAlojado Lamuel Jesu ANo ratings yet
- Clinimetrics Single Assessment Numeric EvaluationDocument1 pageClinimetrics Single Assessment Numeric EvaluationNicol SandovalNo ratings yet
- Excellent Inverters Operation Manual: We Are Your Excellent ChoiceDocument71 pagesExcellent Inverters Operation Manual: We Are Your Excellent ChoicephaPu4cuNo ratings yet
- Polynomials Level 3Document17 pagesPolynomials Level 3greycouncilNo ratings yet
- Head InjuryDocument7 pagesHead InjuryRoshan Ghimire100% (1)
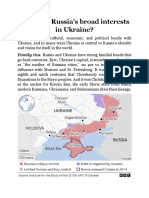
- What Are RussiaDocument3 pagesWhat Are RussiaMuhammad SufyanNo ratings yet
- Rape and Challenging Contemporary ThinkingDocument17 pagesRape and Challenging Contemporary ThinkingKirthna MadhavanNo ratings yet
- Sample Internship PPTDocument19 pagesSample Internship PPTSangeeta JamadarNo ratings yet
- Man Is Made by His BeliefDocument2 pagesMan Is Made by His BeliefLisa KireechevaNo ratings yet