You might also like
- Site Logistics PlanDocument2 pagesSite Logistics Plansampath_priyashantha75% (4)
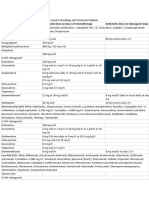
- Drug Adult Dose Child Dose Precautions and ContraindicationsDocument9 pagesDrug Adult Dose Child Dose Precautions and ContraindicationsanshulNo ratings yet
- Motilium PIDocument12 pagesMotilium PIKok Foo YipNo ratings yet
- Lichen PlanusDocument3 pagesLichen PlanusAna PaunescuNo ratings yet
- OsteoporosisDocument15 pagesOsteoporosisWil LesterNo ratings yet
- Docetaxel Carboplatin Trastuzumab T Carbo H Breast Cancer Adjuvant ProtocolDocument14 pagesDocetaxel Carboplatin Trastuzumab T Carbo H Breast Cancer Adjuvant ProtocolsmokkerNo ratings yet
- Common TreatmentsDocument5 pagesCommon TreatmentsRaj MandumulaNo ratings yet
- Prescriptions PDFDocument11 pagesPrescriptions PDFzainolakhNo ratings yet
- Otezla 10 MG Film-Coated Tablets: 1. Name of The Medicinal ProductDocument22 pagesOtezla 10 MG Film-Coated Tablets: 1. Name of The Medicinal ProductSunil SewakNo ratings yet
- Otezla 10 MG Film-Coated Tablets: 1. Name of The Medicinal ProductDocument22 pagesOtezla 10 MG Film-Coated Tablets: 1. Name of The Medicinal ProductSunil SewakNo ratings yet
- Apremilast PI Europe Aug 2019Document14 pagesApremilast PI Europe Aug 2019Wei Sheng ChongNo ratings yet
- Drug Study Ko ToDocument4 pagesDrug Study Ko ToGian Carlo FernandezNo ratings yet
- Ketamine Guidelines Feb 05Document3 pagesKetamine Guidelines Feb 05AdiAri RosiuNo ratings yet
- Class Indications: MetronidazoleDocument3 pagesClass Indications: MetronidazoleDwi WulandariNo ratings yet
- Pharmacology of The Gastrointestinal Drugs (I)Document12 pagesPharmacology of The Gastrointestinal Drugs (I)anaNo ratings yet
- Drug StudyDocument10 pagesDrug StudyFranco ObedozaNo ratings yet
- Flagyl-suspension-SmPC-05.2021 For DistributionDocument9 pagesFlagyl-suspension-SmPC-05.2021 For Distributionrx bafnaNo ratings yet
- Name Mucosta Tablets 100 Description PDFDocument7 pagesName Mucosta Tablets 100 Description PDFnanda RaharjaNo ratings yet
- PCM PoisonDocument23 pagesPCM PoisonPrabhat KcNo ratings yet
- Treatment of Acid-Related Disorders - SeminarDocument40 pagesTreatment of Acid-Related Disorders - SeminarZana Mohammed0% (1)
- Antimalarial Drugs: Varshinidevi V Roll No 92 Ii Yr MbbsDocument37 pagesAntimalarial Drugs: Varshinidevi V Roll No 92 Ii Yr MbbsGoutham MNo ratings yet
- Metoclopramide: GIT Regulators, Antiflatulents & Anti-Inflammatories Antiemetics See Available Brands of MetoclopramideDocument9 pagesMetoclopramide: GIT Regulators, Antiflatulents & Anti-Inflammatories Antiemetics See Available Brands of MetoclopramideDominique RamosNo ratings yet
- Metoclopramide: GIT Regulators, Antiflatulents & Anti-Inflammatories Antiemetics See Available Brands of MetoclopramideDocument9 pagesMetoclopramide: GIT Regulators, Antiflatulents & Anti-Inflammatories Antiemetics See Available Brands of MetoclopramideDominique RamosNo ratings yet
- Nootropil: Qualitative and Quantitative CompositionDocument12 pagesNootropil: Qualitative and Quantitative CompositionMuhammad TalhaNo ratings yet
- L 51 R Hypercvad R MaDocument7 pagesL 51 R Hypercvad R MaMohamed MahmoudNo ratings yet
- Antibioprofilaxia in Ortopedie-TraumatologieDocument22 pagesAntibioprofilaxia in Ortopedie-Traumatologiedocumente.ralucaNo ratings yet
- Motilium: ® Domperidone DatasheetDocument11 pagesMotilium: ® Domperidone DatasheetAurungzaib BhattiNo ratings yet
- Antiamoebic & Other Antiprotozoal DrugsDocument47 pagesAntiamoebic & Other Antiprotozoal DrugsAmit ShahNo ratings yet
- Obat ObgynDocument8 pagesObat ObgynMuhammad Naqiuddin JalaluddinNo ratings yet
- Diabetes Mellitus Drug ChartDocument3 pagesDiabetes Mellitus Drug Chartlui.stephanie1751100% (1)
- Cilastati Imipenem Drug InfoDocument19 pagesCilastati Imipenem Drug InfoCosmina GeorgianaNo ratings yet
- Atacor SPCDocument9 pagesAtacor SPCRannia1No ratings yet
- Metro Nida ZolDocument9 pagesMetro Nida ZolAnna Thalita CardosoNo ratings yet
- Drugs Acting On Gastrointestinal SystemDocument41 pagesDrugs Acting On Gastrointestinal SystemDivya JoyNo ratings yet
- Amitriptyline of My Pharmacology TaskDocument6 pagesAmitriptyline of My Pharmacology TaskRika ChisakaNo ratings yet
- SMILE (Etoposide, Ifosfamide, Methotrexate and Dexamethasone)Document7 pagesSMILE (Etoposide, Ifosfamide, Methotrexate and Dexamethasone)SolikinNo ratings yet
- Mot Ilium TabDocument11 pagesMot Ilium TabChandra FatmaNo ratings yet
- Prescrption WritingDocument47 pagesPrescrption Writingashwarythakur712No ratings yet
- TetracyclinesDocument2 pagesTetracyclinesMariana Mikaela AlagarNo ratings yet
- Algesia: 37.5 MG / 325 MG Film-Coated TABLET AnalgesicDocument1 pageAlgesia: 37.5 MG / 325 MG Film-Coated TABLET AnalgesicEsel WazowskiNo ratings yet
- DMARDs: Uses, ADR and Use in Special SituationsDocument94 pagesDMARDs: Uses, ADR and Use in Special SituationsShoaib MomenNo ratings yet
- AlgesiaDocument1 pageAlgesiaSaf DicamNo ratings yet
- Keterolax Trometamol Classification: Nonsteroidal Anti-Inflamatory DrugDocument7 pagesKeterolax Trometamol Classification: Nonsteroidal Anti-Inflamatory DrugEm Hernandez AranaNo ratings yet
- Management of Gout in AdultsDocument3 pagesManagement of Gout in AdultsZubair Mahmood KamalNo ratings yet
- Chloride: PotassiumDocument6 pagesChloride: PotassiumAseel AlsheeshNo ratings yet
- Diabetes Mellitus Case Study Answers NSDocument4 pagesDiabetes Mellitus Case Study Answers NSShazaan NadeemNo ratings yet
- Emetic Risk of Agents Used in Oncology and TreatmeDocument2 pagesEmetic Risk of Agents Used in Oncology and TreatmeChristina YangNo ratings yet
- Keto LogDocument7 pagesKeto LogKim Justin InfantadoNo ratings yet
- Oseltamivir Indication, Dosage, Side Effect, Precaution MIMS IndonesiaDocument1 pageOseltamivir Indication, Dosage, Side Effect, Precaution MIMS Indonesiaintan alvinnNo ratings yet
- GOUT TherapyDocument7 pagesGOUT TherapyRinda Putri AnggrainiNo ratings yet
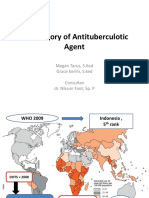
- 1 Category of Antituberculotic Agent: Megan Tarus, S.Ked Grace Kerihi, S.ked Consultan Dr. Nikson Faot, Sp. PDocument10 pages1 Category of Antituberculotic Agent: Megan Tarus, S.Ked Grace Kerihi, S.ked Consultan Dr. Nikson Faot, Sp. PAzrell Albert JonesNo ratings yet
- Mot IliumDocument3 pagesMot IliumLaermie Anne Dichoso MarzanNo ratings yet
- Antiemetics AmoebiasisDocument5 pagesAntiemetics AmoebiasisEaint BoNo ratings yet
- Solian SMPCDocument20 pagesSolian SMPCyanal.bisharat.mspharmaNo ratings yet
- Metformin Hydrochloride PDFDocument4 pagesMetformin Hydrochloride PDFHannaNo ratings yet
- Anti Malarial DrugsDocument42 pagesAnti Malarial DrugsSaurabh GautamNo ratings yet
- Endocrine PrescriptionsDocument41 pagesEndocrine PrescriptionsStock CheckNo ratings yet
- Peptic Ulcer Disease DrugsDocument6 pagesPeptic Ulcer Disease DrugsApple MaeNo ratings yet
- Therapeutic:: Brand Name: PLASIL ClassificationsDocument5 pagesTherapeutic:: Brand Name: PLASIL ClassificationsAbby MontealegreNo ratings yet
- Swine Flu - Read About Symptoms, Treatment and H1N1 VaccineDocument10 pagesSwine Flu - Read About Symptoms, Treatment and H1N1 VaccineRoyal ENo ratings yet
- The 2030 Agenda For Sustainable Development and The "Five PS"Document2 pagesThe 2030 Agenda For Sustainable Development and The "Five PS"Laraib ShahidNo ratings yet
- Common Course Outline For: EXSC 2305 Exercise Physiology A. Course DescriptionDocument2 pagesCommon Course Outline For: EXSC 2305 Exercise Physiology A. Course DescriptionZedy GullesNo ratings yet
- KAR Products - Gloss White Aerosol PaintDocument7 pagesKAR Products - Gloss White Aerosol Paintjaredf@jfelectric.comNo ratings yet
- Delta Model 31 080 1 Belt Sander ManualDocument12 pagesDelta Model 31 080 1 Belt Sander ManualJon LewisNo ratings yet
- Thought Field TherapyDocument5 pagesThought Field TherapyMitz VinegasNo ratings yet
- Practice Station History Breathless 1Document8 pagesPractice Station History Breathless 1Wenbin GuoNo ratings yet
- Pharmaceutical Jurisprudence Sovan Sarkar 186012111012Document11 pagesPharmaceutical Jurisprudence Sovan Sarkar 186012111012Sovan SarkarNo ratings yet
- Lab Clin Clin Tasks Attempted 1 2 3 4 5 6 7: ST ND RD TH TH TH THDocument4 pagesLab Clin Clin Tasks Attempted 1 2 3 4 5 6 7: ST ND RD TH TH TH THRichard Patterson100% (1)
- United Nations For Class 8Document36 pagesUnited Nations For Class 8zeeschool25% (4)
- (1998) Chronic Disease Management What Will It Take To Improve Care For Chronic IllnessDocument3 pages(1998) Chronic Disease Management What Will It Take To Improve Care For Chronic IllnessDaniel MeloNo ratings yet
- Vasculitis SyndromesDocument56 pagesVasculitis SyndromesHengki Permana PutraNo ratings yet
- Aviation Laser Exposure Self-Assessment PDFDocument2 pagesAviation Laser Exposure Self-Assessment PDFmimiNo ratings yet
- Vademecum Eiffel 2019 en PDFDocument8 pagesVademecum Eiffel 2019 en PDFMais OmarNo ratings yet
- Polysomnograph EnglishDocument5 pagesPolysomnograph EnglishRam BehinNo ratings yet
- Brihat Dadimashtaka ChurnaDocument6 pagesBrihat Dadimashtaka ChurnaSamhitha Ayurvedic Chennai100% (1)
- Cases Toxo & ForensicDocument27 pagesCases Toxo & ForensicAhmed MohamedNo ratings yet
- Hbsag Form New 2021Document1 pageHbsag Form New 2021GCMDHNo ratings yet
- Report #5 (Tomás Castro)Document26 pagesReport #5 (Tomás Castro)Tomas Castro D SantosNo ratings yet
- Rebeccas Resume Updated 7-2016Document1 pageRebeccas Resume Updated 7-2016api-498987425No ratings yet
- 04 2022 Chicha PDRRMODocument6 pages04 2022 Chicha PDRRMOmikko parelNo ratings yet
- Statement Uni - SenithaDocument2 pagesStatement Uni - SenithaSenitha MindulaNo ratings yet
- Drug List 1Document2 pagesDrug List 1Ezra Lee NgatiyonNo ratings yet
- DRRM Toolkit Book - Final PDFDocument379 pagesDRRM Toolkit Book - Final PDFAnonymous JLQBb3JNo ratings yet
- Dyspepsia On CommonDocument21 pagesDyspepsia On CommonChatrina TandiloloNo ratings yet
- Experiment: Analysis of Milk: Output by Christian James MataDocument2 pagesExperiment: Analysis of Milk: Output by Christian James MataSIJINo ratings yet
- Circles of SupportDocument1 pageCircles of Supportapi-276867030No ratings yet
- VPHin IndiaoieproofDocument17 pagesVPHin Indiaoieproofhari prasadNo ratings yet
- Anxiety Disorders and Their Treatment Antony-Swinson-1996Document123 pagesAnxiety Disorders and Their Treatment Antony-Swinson-1996Ruxandra CraciunNo ratings yet