You might also like
- Patholgy Final BcqsDocument74 pagesPatholgy Final BcqsMaryam KhalidNo ratings yet
- BLOOD MCQsDocument27 pagesBLOOD MCQstyno Majon100% (3)
- Pathology-MCQs - PDF Copy CopyDocument130 pagesPathology-MCQs - PDF Copy CopyMhamad MamasenyNo ratings yet
- Genral Path MCQDocument171 pagesGenral Path MCQAbir AlamNo ratings yet
- Book Back MCQDocument51 pagesBook Back MCQClinton ThomasNo ratings yet
- MCQ 2Document22 pagesMCQ 2Mohmmad WhaidyNo ratings yet
- Phsio EXITABLEDocument12 pagesPhsio EXITABLEmohammedNo ratings yet
- Cellular InjuryDocument26 pagesCellular InjuryRitz CelsoNo ratings yet
- 4 2 PDFDocument9 pages4 2 PDFMahtab KhalifpourNo ratings yet
- ImmunologyDocument3 pagesImmunologybhawana bhattNo ratings yet
- Neoplasia From Med Geek PDFDocument30 pagesNeoplasia From Med Geek PDFTony DawaNo ratings yet
- Pooled Mcqs For Gre/Gat/Subject Discipline: (Pathology)Document61 pagesPooled Mcqs For Gre/Gat/Subject Discipline: (Pathology)Faizan AliNo ratings yet
- PathoDocument12 pagesPathoola nagarNo ratings yet
- PreTest - Pathology Questions Multiple Choice Sample ExamDocument23 pagesPreTest - Pathology Questions Multiple Choice Sample ExamAdmin DutiesNo ratings yet
- GENPATHODocument4 pagesGENPATHOMitch C.No ratings yet
- ExamDocument70 pagesExamAyman RagabNo ratings yet
- Final ExamsDocument16 pagesFinal ExamsSadru Prince SnigleNo ratings yet
- MBBS Pathology MCQsDocument4 pagesMBBS Pathology MCQsDoctorAlan John Naveen Chandar100% (2)
- PHS MCQ Tutorials 200lDocument4 pagesPHS MCQ Tutorials 200lcollinsmagNo ratings yet
- Identify The Choice That Best Completes The Statement or Answers The QuestionDocument14 pagesIdentify The Choice That Best Completes The Statement or Answers The QuestionCamille BaybayNo ratings yet
- Module 3 PhysiologyDocument11 pagesModule 3 PhysiologyDasun J.100% (1)
- Review Mcqs For 2016 Systemic PathologyDocument8 pagesReview Mcqs For 2016 Systemic PathologySameer100% (1)
- BSN 214 Pathology Exam (00000003)Document7 pagesBSN 214 Pathology Exam (00000003)NatalyaNo ratings yet
- MCQ Part 1 2005 "Example Questions"Document3 pagesMCQ Part 1 2005 "Example Questions"RayC1977No ratings yet
- Tropical MCQS: C. Visceral LeishmaniasisDocument29 pagesTropical MCQS: C. Visceral Leishmaniasisساره ابوالقاسمNo ratings yet
- 004 Pathology MCQ ACEM Primary CellularDocument3 pages004 Pathology MCQ ACEM Primary Cellularbmhsh100% (1)
- Hemodynamic DisordersDocument6 pagesHemodynamic DisordersPradeep100% (1)
- Acute and Chronic Inflammation MCQDocument2 pagesAcute and Chronic Inflammation MCQPrahul100% (1)
- RBC DiorderDocument13 pagesRBC DiorderHabib UllahNo ratings yet
- Microbiology Mcqs 1Document9 pagesMicrobiology Mcqs 1Patricia Denise OrquiaNo ratings yet
- REVIEW Cell Adaptation, Injury and DeathDocument101 pagesREVIEW Cell Adaptation, Injury and DeathandiariansyahNo ratings yet
- PATHOLOGYDocument10 pagesPATHOLOGYDivine SangutanNo ratings yet
- Module 1. General and Special Questions of Clinical Laboratory Diagnostics Text Test QuestionDocument229 pagesModule 1. General and Special Questions of Clinical Laboratory Diagnostics Text Test QuestionA.h.MuradNo ratings yet
- GP Micro MCQ PDFDocument8 pagesGP Micro MCQ PDFAnna CortiNo ratings yet
- Select The Single Best Answer of The Following:: B. Non-ImmunogenicDocument14 pagesSelect The Single Best Answer of The Following:: B. Non-ImmunogenicAdel AlomarNo ratings yet
- Topics of Systematic Pathology (To Be Taught in The Second Term)Document8 pagesTopics of Systematic Pathology (To Be Taught in The Second Term)Gamal DawoodNo ratings yet
- Study Guide For Lecture Exam 2 Biol 1407 03.12.2010Document50 pagesStudy Guide For Lecture Exam 2 Biol 1407 03.12.2010Erica MizzIndependent BubuchuNo ratings yet
- General Pathology Saq Sample Exam eDocument7 pagesGeneral Pathology Saq Sample Exam eRIZ KHANNo ratings yet
- Chapter 01 - Anatomy and Electrophysiology of The Heart: Multiple Choice QuestionsDocument17 pagesChapter 01 - Anatomy and Electrophysiology of The Heart: Multiple Choice QuestionsyebegashetNo ratings yet
- Helm in TH OlogyDocument42 pagesHelm in TH OlogyNiaz Asghar75% (4)
- Spleen MCQDocument22 pagesSpleen MCQShriyansh Chahar0% (1)
- QuizDocument16 pagesQuizSiriporn PongpattarapakNo ratings yet
- Pathology RevisionDocument43 pagesPathology RevisionjayNo ratings yet
- Neoplasia QuizDocument9 pagesNeoplasia QuizBrother GeorgeNo ratings yet
- Pathology Exam Committee VDocument7 pagesPathology Exam Committee VErsin TukenmezNo ratings yet
- Acute InflammationDocument64 pagesAcute InflammationSuleiman KikulweNo ratings yet
- Histopathology MCQDocument4 pagesHistopathology MCQkennethakpo61No ratings yet
- Immunology Mid-ExamDocument11 pagesImmunology Mid-ExamNgMinhHaiNo ratings yet
- Chapter 03 - Inflammation and Tissue RepairDocument7 pagesChapter 03 - Inflammation and Tissue RepairJo100% (2)
- Hemodynamic MCQ From GhadeerDocument3 pagesHemodynamic MCQ From GhadeerKehkashan Khan100% (1)
- Which of The Following Tumors May Contain A Cartilaginous ComponentDocument12 pagesWhich of The Following Tumors May Contain A Cartilaginous ComponentKayeNo ratings yet
- Neoplasia ExamDocument9 pagesNeoplasia ExamYheng Gaosaii100% (1)
- Test 3 BDSDocument16 pagesTest 3 BDSrababNo ratings yet
- CVS Irfan HabibDocument6 pagesCVS Irfan HabibPardeep Dhurgesh Nkh RatananiNo ratings yet
- Two-Dimensional Gel Electrophoresis of Proteins: Methods and ApplicationsFrom EverandTwo-Dimensional Gel Electrophoresis of Proteins: Methods and ApplicationsJulio CelisNo ratings yet
- Quiz PathologyDocument28 pagesQuiz PathologyMedShare86% (35)
- Patho ExamDocument16 pagesPatho ExamIbrahim BarhamNo ratings yet
- Hematology MCQsDocument84 pagesHematology MCQsHyder Ali84% (19)
- Chapter 1 Compiled General Pathology QuestionsDocument14 pagesChapter 1 Compiled General Pathology Questionsvetpathforum90% (10)
- IFLA HIV AIDS WorkshopDocument17 pagesIFLA HIV AIDS WorkshopMunish DograNo ratings yet
- Parenthood Is FascinatingDocument2 pagesParenthood Is FascinatingMunish DograNo ratings yet
- Malabsorption A Clinical ApproachDocument42 pagesMalabsorption A Clinical ApproachMunish DograNo ratings yet
- Risk AnalysisDocument50 pagesRisk AnalysisMunish DograNo ratings yet
- Radiation HazardsDocument32 pagesRadiation HazardsMunish DograNo ratings yet
- Ionising Radiation and Living ThingsDocument23 pagesIonising Radiation and Living ThingsMunish DograNo ratings yet
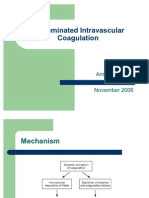
- Disseminated Intravascular CoagulationDocument12 pagesDisseminated Intravascular CoagulationMunish Dogra100% (1)
- Corporate ApartheidDocument4 pagesCorporate ApartheidMunish DograNo ratings yet
- Once You Have Decided To Start An NGODocument3 pagesOnce You Have Decided To Start An NGOMunish DograNo ratings yet
- Human Anatomy & PhysiologyDocument100 pagesHuman Anatomy & PhysiologyMunish DograNo ratings yet
- India Education TrendsDocument3 pagesIndia Education TrendsMunish DograNo ratings yet
- THALASSEMIADocument49 pagesTHALASSEMIAMunish DograNo ratings yet
- Fight For Freedom: Ancient Liberalism of MaterialismDocument4 pagesFight For Freedom: Ancient Liberalism of MaterialismMunish DograNo ratings yet
- Every Child Is SpecialDocument1 pageEvery Child Is SpecialMunish DograNo ratings yet
- Ambushed After They Saw Off Colleagues Going On LeaveDocument2 pagesAmbushed After They Saw Off Colleagues Going On LeaveMunish DograNo ratings yet
- It's Bureaucracy Vs PoliticsDocument2 pagesIt's Bureaucracy Vs PoliticsMunish DograNo ratings yet
- New Engines of Social ChangeDocument3 pagesNew Engines of Social ChangeMunish DograNo ratings yet
- 9 Sports Movies Women LoveDocument3 pages9 Sports Movies Women LoveMunish DograNo ratings yet
- Arundhati RoyDocument2 pagesArundhati RoyMunish DograNo ratings yet
- Lupus Erythematosus CellDocument58 pagesLupus Erythematosus CellMunish Dogra100% (1)
- Radiation HazardsDocument40 pagesRadiation HazardsMunish Dogra100% (1)
- Triple Screening Test.Document2 pagesTriple Screening Test.Munish DograNo ratings yet
- Hematoxylin Stain Its Importance in HistologyDocument35 pagesHematoxylin Stain Its Importance in HistologyMunish Dogra75% (4)
- High Voltage X-Ray GeneratorDocument52 pagesHigh Voltage X-Ray GeneratorMunish Dogra100% (3)
- Coombs' TestDocument42 pagesCoombs' TestMunish Dogra100% (1)
- Dengue Pathogenesis and DiagnosisDocument45 pagesDengue Pathogenesis and DiagnosisMunish DograNo ratings yet
- Bone Marrow Strcuture and FunctionDocument25 pagesBone Marrow Strcuture and FunctionMunish DograNo ratings yet
- Chest RadiographyDocument65 pagesChest RadiographyMunish Dogra100% (1)
- Bone Marrow TransplantDocument17 pagesBone Marrow TransplantMunish Dogra100% (1)
- Compatibility Testing For Blood TransfusionDocument40 pagesCompatibility Testing For Blood TransfusionMunish Dogra100% (4)
- Widoasti Putri Utami - 22010120410005 PDFDocument20 pagesWidoasti Putri Utami - 22010120410005 PDFdevaNo ratings yet
- Bone BiochemistryDocument21 pagesBone BiochemistrySheilasmNo ratings yet
- CH 07Document46 pagesCH 07abdurNo ratings yet
- BIO122 - CHAPTER 7 Part 1Document53 pagesBIO122 - CHAPTER 7 Part 1lili100% (1)
- What Affects The Biocompatibility of PolymersDocument25 pagesWhat Affects The Biocompatibility of PolymersAndreaNo ratings yet
- Artigo MiriamDocument23 pagesArtigo MiriamDiego Alfonso Arregui RamosNo ratings yet
- Bok:978 1 4614 9434 8 PDFDocument700 pagesBok:978 1 4614 9434 8 PDFCRISTOBAL BESNIERNo ratings yet
- Effect of Hyaluronic Acid On The Osseointegration of Dental ImplantsDocument5 pagesEffect of Hyaluronic Acid On The Osseointegration of Dental Implantsjaviers45No ratings yet
- Cartilage & BoneDocument8 pagesCartilage & BoneRehab OmerNo ratings yet
- USMLE Step 1 GuideDocument13 pagesUSMLE Step 1 Guidegemazy123100% (3)
- Extracellular Matrix For Tissue Engineering and Biomaterials PDFDocument218 pagesExtracellular Matrix For Tissue Engineering and Biomaterials PDFhuldani-1No ratings yet
- Development of Human PeriodontiumDocument117 pagesDevelopment of Human PeriodontiumvsdeepsNo ratings yet
- Effect of Astaxanthin On Cutaneous Wound Healing: Clinical, Cosmetic and Investigational Dermatology DoveDocument7 pagesEffect of Astaxanthin On Cutaneous Wound Healing: Clinical, Cosmetic and Investigational Dermatology DoveRaziel Alvarez RebolloNo ratings yet
- The Significance of Complex Polysaccharides in Personal Care FormulationsDocument22 pagesThe Significance of Complex Polysaccharides in Personal Care FormulationsMathieu VigneauNo ratings yet
- Form and Function of The Meniscus: Scott A. Rodeo, MD Sumito Kawamura, MDDocument16 pagesForm and Function of The Meniscus: Scott A. Rodeo, MD Sumito Kawamura, MDIkre19No ratings yet
- Study Guide-Axon Guidance 1Document2 pagesStudy Guide-Axon Guidance 1joeyNo ratings yet
- Biomechanics of Articular CartilageDocument33 pagesBiomechanics of Articular CartilageLibbyNo ratings yet
- NeoplasiaDocument78 pagesNeoplasiageetikaNo ratings yet
- Properties of Soft Tissue-: Response To Immobilization and StretchDocument55 pagesProperties of Soft Tissue-: Response To Immobilization and StretchSneha Makwana50% (2)
- PDFDocument16 pagesPDFĐặng HươngNo ratings yet
- J Jacc 2007 02 059v1Document17 pagesJ Jacc 2007 02 059v1maestro1234567890No ratings yet
- HBT Always Young Kırışıklık Kremi Klinik Analiz Laboratuvar SonuçlarıDocument12 pagesHBT Always Young Kırışıklık Kremi Klinik Analiz Laboratuvar SonuçlarıHakanNo ratings yet
- Active Series: Grant Industries, IncDocument20 pagesActive Series: Grant Industries, IncechoNo ratings yet
- The Wound Healing ProcessDocument15 pagesThe Wound Healing Processtabris76No ratings yet
- 3D Cell Culture in Alginate HydrogelsDocument29 pages3D Cell Culture in Alginate Hydrogelslolitica123456No ratings yet
- 3 Interview Transcripts From The Body Electric Summit 2 0 From Christine Schaffner NDDocument42 pages3 Interview Transcripts From The Body Electric Summit 2 0 From Christine Schaffner NDAndre3893100% (1)
- MucopolysaccharidesDocument19 pagesMucopolysaccharidesUmar Jutt100% (2)
- Introduction To HistologyDocument34 pagesIntroduction To HistologyAnonymous B5CaVOAt100% (1)
- Biotechnology AdvancesDocument24 pagesBiotechnology AdvancesKhaled Al GhaebNo ratings yet
- Microcarrier Cell Culture ScaleUp Procedures HandbookDocument32 pagesMicrocarrier Cell Culture ScaleUp Procedures HandbookDolphingNo ratings yet