You might also like
- CDNDocument2 pagesCDNJohn Paulo MoralesNo ratings yet
- Chickenpox & ChlamydialDocument5 pagesChickenpox & ChlamydialEliezah RodriguezNo ratings yet
- Case Study in Micro-1Document50 pagesCase Study in Micro-1Angie Cabanting BañezNo ratings yet
- Viral InfectionsDocument34 pagesViral InfectionsAlaa MadmoujNo ratings yet
- 3.torch InfectionsDocument15 pages3.torch InfectionsKuleshwar SahuNo ratings yet
- Sexually Transmitted Infections and PregnancyDocument19 pagesSexually Transmitted Infections and PregnancyBeyins TiuNo ratings yet
- Communicable Diseases Affecting The Reproductive SystemDocument49 pagesCommunicable Diseases Affecting The Reproductive SystemJR Rolf NeuqeletNo ratings yet
- ScabiesDocument16 pagesScabiescarla_sarmiento4847No ratings yet
- Childhood Sicknesses1111Document17 pagesChildhood Sicknesses1111abdulrahmanbelewa96No ratings yet
- Clinical ManifestationDocument6 pagesClinical ManifestationKrystal Jane SalinasNo ratings yet
- Name: Carlo M. Yao Bachelor of Science in NursingDocument33 pagesName: Carlo M. Yao Bachelor of Science in Nursingcarlo24_briggsNo ratings yet
- Measles (Report) DocsDocument4 pagesMeasles (Report) DocsCrystal AbarrientosNo ratings yet
- Dengue 1Document6 pagesDengue 1Johannah Ruth BacolodNo ratings yet
- Viral Diseases - 06Document51 pagesViral Diseases - 06HIMANSHU SINGHNo ratings yet
- SARS-2nd ProffDocument27 pagesSARS-2nd ProffMuhammad aslamNo ratings yet
- Psoriasis: Posted: 02 Aug 2010 11:18 PM PDTDocument5 pagesPsoriasis: Posted: 02 Aug 2010 11:18 PM PDTScamb TrekNo ratings yet
- ChickenpoxDocument4 pagesChickenpoxJen Vizcarra CaminoNo ratings yet
- Measles (Rubeola) Rubeola Red Spot: Dr. Eman Khammas Alsadi Community Medicine LecturerDocument34 pagesMeasles (Rubeola) Rubeola Red Spot: Dr. Eman Khammas Alsadi Community Medicine Lecturereman khammasNo ratings yet
- Chicken-Pox Concept MapDocument4 pagesChicken-Pox Concept MapElle0% (1)
- Mayores. Chicken Pox - Concept MapDocument3 pagesMayores. Chicken Pox - Concept MapAlvic Dy KowNo ratings yet
- Synonyms Causative Agents Incubatiob Period Mode of Transmission Signs and Symptoms Period of Communicability Diagnostic Test Medical Management Nursing Management ComplicationsDocument13 pagesSynonyms Causative Agents Incubatiob Period Mode of Transmission Signs and Symptoms Period of Communicability Diagnostic Test Medical Management Nursing Management ComplicationsYnah DominiqueNo ratings yet
- LECTURE 02A German MeaslesDocument21 pagesLECTURE 02A German Measlesraxma4682No ratings yet
- Chicken PoxDocument4 pagesChicken PoxFloyd SevillaNo ratings yet
- School PrerequistesDocument65 pagesSchool Prerequistesmanaribrahim309No ratings yet
- Https://ar - scribd.com/document/391648283/OET Future Land Full Book Final Edition July 2018Document52 pagesHttps://ar - scribd.com/document/391648283/OET Future Land Full Book Final Edition July 2018Qutaiba ShdaifatNo ratings yet
- 2 - SyphilisDocument24 pages2 - SyphilisCaila LimNo ratings yet
- Signs and SymptomsDocument6 pagesSigns and SymptomsKajim SharibiNo ratings yet
- PAEDS 4 - 18.10.19 Viral InfectionDocument15 pagesPAEDS 4 - 18.10.19 Viral Infectionlotp12No ratings yet
- Chickenpox ActividadDocument6 pagesChickenpox ActividadAngie MinayaNo ratings yet
- Sexually Transmitted DiseasesDocument17 pagesSexually Transmitted DiseasesChrystele Ann Ramilo100% (1)
- CHN - Communicable DiseaseDocument117 pagesCHN - Communicable DiseaseGetom NgukirNo ratings yet
- Herpes 3, VSVDocument21 pagesHerpes 3, VSVCharles SainzNo ratings yet
- Kutis PorcelanaDocument34 pagesKutis Porcelanaapi-3743483No ratings yet
- Child Health Nursing: MumpsDocument25 pagesChild Health Nursing: MumpsmanibharathiNo ratings yet
- UntitledDocument6 pagesUntitledGenelly Anne Argañoza RamosNo ratings yet
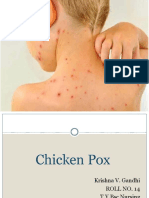
- Chicken PoxDocument26 pagesChicken PoxKrishna GandhiNo ratings yet
- Monkeypox RA and MX 27 Mei 2022Document45 pagesMonkeypox RA and MX 27 Mei 2022alfonso de albuquerqueNo ratings yet
- Sexually Transmitted DiseasesDocument19 pagesSexually Transmitted DiseasesAhmed HajiNo ratings yet
- ChickenpoxDocument24 pagesChickenpoxPRATIK SHRESTHANo ratings yet
- Vulvovaginitis in Childhood: Cristina Vezzani, Gilda Di Paolo, Terryann Spagnuolo, and Gabriele TridentiDocument17 pagesVulvovaginitis in Childhood: Cristina Vezzani, Gilda Di Paolo, Terryann Spagnuolo, and Gabriele TridentiIvonne CabreraNo ratings yet
- Gusti Izza - English Medical ArticleDocument6 pagesGusti Izza - English Medical Articlenuna_idaNo ratings yet
- 1-Measles (Rubeola) PDFDocument37 pages1-Measles (Rubeola) PDFمصطفى رسول هاديNo ratings yet
- Medical Terms Kind of IlnessDocument11 pagesMedical Terms Kind of IlnessFani KimerliNo ratings yet
- Chickenpox: SymptomsDocument10 pagesChickenpox: SymptomsAnand SwamiNo ratings yet
- VaricellachickenpoxDocument6 pagesVaricellachickenpoxDedi SofyanNo ratings yet
- Genitourinary SystemDocument7 pagesGenitourinary SystemMary Angel VelascoNo ratings yet
- Lect 4 Viral InfectionDocument44 pagesLect 4 Viral InfectionAMIT GUPTANo ratings yet
- Meehleib, Rachelle Ayn S. Pepino, Stephanie Kate ADocument16 pagesMeehleib, Rachelle Ayn S. Pepino, Stephanie Kate ARachelle AynNo ratings yet
- Helminths (Tapeworm, Pinworm) - NavarroDocument26 pagesHelminths (Tapeworm, Pinworm) - NavarroThaddeus Dalagan NavarroNo ratings yet
- Acute Infections During PregnancyDocument63 pagesAcute Infections During PregnancyHussein AliNo ratings yet
- Rle BSN 2 (Lesson 3) (2021-2022)Document26 pagesRle BSN 2 (Lesson 3) (2021-2022)Flonamae AbiarNo ratings yet
- WCLF E1 J 66 F YPUTf 0149Document165 pagesWCLF E1 J 66 F YPUTf 0149ClintonNo ratings yet
- MEASLES and MALARIADocument19 pagesMEASLES and MALARIADoreen Claire M. WallangNo ratings yet
- Common DiseasesDocument7 pagesCommon DiseasesAlter BadonNo ratings yet
- GonorrheaDocument22 pagesGonorrheaSharah Londonio100% (1)
- Sexually Transmitted Diseases: Jasmin P. EgargueDocument33 pagesSexually Transmitted Diseases: Jasmin P. EgargueLiza AingelicaNo ratings yet
- Monkey Pox FinalDocument35 pagesMonkey Pox FinalHiren patelNo ratings yet
- ChickenpoxDocument7 pagesChickenpoxJennevy Buque100% (1)
- CHN DiseasesDocument216 pagesCHN DiseasesCzarina May TumandanNo ratings yet
- JN KDocument24 pagesJN Kcatch.amit19No ratings yet
- Pascual V PascualDocument2 pagesPascual V PascualAices SalvadorNo ratings yet
- Population Disadvantage GDI 2005Document71 pagesPopulation Disadvantage GDI 2005Incoherency100% (12)
- Open Fire Assembly GuidesDocument2 pagesOpen Fire Assembly GuidesRandall CaseNo ratings yet
- An Introduction To Historical "Lavender" Linguistics byDocument2 pagesAn Introduction To Historical "Lavender" Linguistics byapi-25885198No ratings yet
- 47 - Ong Vs CA, GR 95386, May 29, 1997Document6 pages47 - Ong Vs CA, GR 95386, May 29, 1997美咲剛No ratings yet
- Passive SentencesDocument6 pagesPassive SentencesFadiaNo ratings yet
- M.A. in Social Work Colleges in North IndiaDocument2 pagesM.A. in Social Work Colleges in North Indiasandeepkumarmsw8442No ratings yet
- 0 042010 Notes - Brandon AdamsDocument17 pages0 042010 Notes - Brandon AdamsCK in DC100% (5)
- EM 8-Position PaperDocument2 pagesEM 8-Position PaperSTEVEN MENDEZNo ratings yet
- Motion For Stay Pending Appeal and Memo in SupportDocument15 pagesMotion For Stay Pending Appeal and Memo in SupportMartin AustermuhleNo ratings yet
- Space Opera Adv - 1Document24 pagesSpace Opera Adv - 1Jacopo Jbb ColabattistaNo ratings yet
- An Example of Narrative TextDocument2 pagesAn Example of Narrative TextihdaNo ratings yet
- Enquiry ProceedingsDocument5 pagesEnquiry ProceedingsNiraj Kumar MishraNo ratings yet
- Jail (Prison Constable Merit) - 1Document419 pagesJail (Prison Constable Merit) - 1Mujeeb Ur RehmanNo ratings yet
- Article 7 Sec 4 Legarda V de CastroDocument2 pagesArticle 7 Sec 4 Legarda V de CastroJc Araojo100% (1)
- Drug Law Enforcement: Narcotics Control BureauDocument160 pagesDrug Law Enforcement: Narcotics Control BureausameerNo ratings yet
- Framework For Conflict AnalysisDocument18 pagesFramework For Conflict Analysiseliasox123No ratings yet
- EXAMINING THE ROLE OF THE 50/50 GROUP Thesis From FredlineDocument209 pagesEXAMINING THE ROLE OF THE 50/50 GROUP Thesis From FredlineBrima GeorgeNo ratings yet
- 4 G.R. No. 171673 Banahaw vs. PacanaDocument8 pages4 G.R. No. 171673 Banahaw vs. Pacanaaags_06No ratings yet
- Digital Devils - Player AgreementDocument3 pagesDigital Devils - Player AgreementRizaNo ratings yet
- Nuestra Senora de La Inmaculada Concepcion y Del Triunfo de La Cruz de MigpangiDocument2 pagesNuestra Senora de La Inmaculada Concepcion y Del Triunfo de La Cruz de MigpangilhemnavalNo ratings yet
- Prime Marine Service vs. NLRC DDocument3 pagesPrime Marine Service vs. NLRC DCzar Ian AgbayaniNo ratings yet
- SIRD MizoramDocument2 pagesSIRD MizoramRaju MacharlaNo ratings yet
- Recognition of Foreign Divorce in The PhilippinesDocument9 pagesRecognition of Foreign Divorce in The PhilippinesRaffy Pangilinan0% (1)
- Report of The African Court On Human and Peoples Rights in The Protection of Human Rights in Africa FinalDocument10 pagesReport of The African Court On Human and Peoples Rights in The Protection of Human Rights in Africa FinalRANDAN SADIQNo ratings yet
- International Express Travel v. CADocument3 pagesInternational Express Travel v. CACherry ChaoNo ratings yet
- Holocaust Era Assets Conference Proceedings 2009Document653 pagesHolocaust Era Assets Conference Proceedings 2009bekowiczNo ratings yet
- Gogol, Eugene - Toward A Dialectic of Philosophy and OrganizationDocument409 pagesGogol, Eugene - Toward A Dialectic of Philosophy and Organizationzvonomir100% (1)
- Airport Activities VocabularyDocument3 pagesAirport Activities VocabularyTY FlamencoSNo ratings yet