You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Occupational Lung DiseaseDocument31 pagesOccupational Lung DiseaseRapid Medicine100% (2)
- Tutorial Neuro Part II... : by KTDocument54 pagesTutorial Neuro Part II... : by KTRapid Medicine100% (1)
- MCQ R2Document241 pagesMCQ R2Rapid Medicine100% (3)
- ClassicDocument4 pagesClassicReggie Ann S. PolicarpioNo ratings yet
- Nephrology TestDocument112 pagesNephrology TestRapid Medicine50% (2)
- SpondyloarthritisDocument77 pagesSpondyloarthritisRapid MedicineNo ratings yet
- Vasculitis JeabnoiiDocument57 pagesVasculitis JeabnoiiRapid Medicine100% (2)
- 23 May 2011 Peerapat Thaisiam Yossavadee RuamcharoenDocument109 pages23 May 2011 Peerapat Thaisiam Yossavadee RuamcharoenRapid MedicineNo ratings yet
- Current Graves' Disease - THPKDocument60 pagesCurrent Graves' Disease - THPKRapid MedicineNo ratings yet
- Cluster HeadacheDocument34 pagesCluster HeadacheRapid MedicineNo ratings yet
- Approach in Endocrine DiseaseDocument32 pagesApproach in Endocrine DiseaseRapid Medicine83% (6)
- Approach in GI-HBDocument19 pagesApproach in GI-HBRapid Medicine100% (2)
- Approach in NeurologyDocument29 pagesApproach in NeurologyRapid Medicine100% (4)
- Approach in HematologyDocument6 pagesApproach in HematologyRapid Medicine67% (3)
- Approach in MiscellaneousDocument12 pagesApproach in MiscellaneousRapid MedicineNo ratings yet
- Survival in Long CaseDocument7 pagesSurvival in Long CaseRapid MedicineNo ratings yet
- Survival in Long CaseDocument7 pagesSurvival in Long CaseRapid MedicineNo ratings yet
- Basic CTDocument71 pagesBasic CTRapid Medicine100% (2)
- Infective Endocarditis: Uaepong Limpapanasit July 5, 2010Document45 pagesInfective Endocarditis: Uaepong Limpapanasit July 5, 2010Rapid MedicineNo ratings yet
- Nontuberculous Mycobacterial Diseases: Nitiwat Chansuk Internal Medicine KKU July, 4 2011Document55 pagesNontuberculous Mycobacterial Diseases: Nitiwat Chansuk Internal Medicine KKU July, 4 2011Rapid MedicineNo ratings yet
- พี่พงษ์ติวcardioDocument79 pagesพี่พงษ์ติวcardioRapid Medicine67% (3)
- NeuroShort Cases 05 04Document63 pagesNeuroShort Cases 05 04Rapid MedicineNo ratings yet
- Foot DropDocument10 pagesFoot DropRapid Medicine100% (1)
- Thyroiditis: Uaepong Limpapanasit 23/5/54Document36 pagesThyroiditis: Uaepong Limpapanasit 23/5/54Rapid MedicineNo ratings yet
- film rheumato-2 พี่เอDocument48 pagesfilm rheumato-2 พี่เอRapid MedicineNo ratings yet
- Rheum A To Logy Tutorial HandoutDocument12 pagesRheum A To Logy Tutorial HandoutRapid Medicine100% (1)
- Siam ID Board Review 2010Document41 pagesSiam ID Board Review 2010Rapid Medicine100% (1)
- Ms-Kku 24-09-2009Document134 pagesMs-Kku 24-09-2009Rapid MedicineNo ratings yet
- Lectures VasculitisDocument29 pagesLectures VasculitisRapid Medicine100% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- About The Series - Read MeDocument4 pagesAbout The Series - Read MejlhotaruNo ratings yet
- Acute Rheumatic FeverDocument51 pagesAcute Rheumatic FeverFaedil Ichsan CiremaiNo ratings yet
- Newsday 09042020 PDFDocument16 pagesNewsday 09042020 PDFKennedy Dube100% (1)
- Blood Transfusion ENGLISHDocument40 pagesBlood Transfusion ENGLISHHajrahPalembangan100% (2)
- Health Center - PaterosDocument5 pagesHealth Center - PaterosmawaaahNo ratings yet
- NT Health Factsheet On HTLV-1 For CliniciansDocument2 pagesNT Health Factsheet On HTLV-1 For CliniciansSBS_NewsNo ratings yet
- CarbohydratesDocument3 pagesCarbohydratesRheaNo ratings yet
- Daftar PustakaDocument5 pagesDaftar PustakaGeraldo Primaman CoffeeNo ratings yet
- OSCE Master List - CardiologyDocument10 pagesOSCE Master List - CardiologyRebecca WongNo ratings yet
- Molecular Biology Module 5 (Oncogenes)Document5 pagesMolecular Biology Module 5 (Oncogenes)sag12344321No ratings yet
- Poultry DiseaseDocument8 pagesPoultry DiseaseJoão Silva0% (1)
- Firs World Report PDFDocument35 pagesFirs World Report PDFMarv MarvNo ratings yet
- Avian Influenza (Highly Pathogenic) : Fowl Plague, Fowl Pest, Brunswick Bird Plague, Fowl Disease, Fowl or Bird GrippeDocument23 pagesAvian Influenza (Highly Pathogenic) : Fowl Plague, Fowl Pest, Brunswick Bird Plague, Fowl Disease, Fowl or Bird Grippehericonan9No ratings yet
- Assignment Benu 4131Document2 pagesAssignment Benu 4131SmileNo ratings yet
- 07-Acute Diarrheal Diseases (Ward Lectures)Document33 pages07-Acute Diarrheal Diseases (Ward Lectures)Zaryab Umar100% (1)
- ACP (American College of Physicians) Medicine-2006 PDFDocument3,054 pagesACP (American College of Physicians) Medicine-2006 PDFPuskesmasmedandenaiNo ratings yet
- History of Present IllnessDocument2 pagesHistory of Present IllnessReylan GarciaNo ratings yet
- The Philippines in World of PandemicDocument18 pagesThe Philippines in World of PandemicDon QuixoteNo ratings yet
- Lecture Notes On Public HealthDocument342 pagesLecture Notes On Public Healthredroseeeeee67% (3)
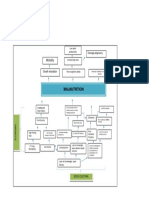
- Problem Tree Analysis MalnutritionDocument1 pageProblem Tree Analysis MalnutritionMho Dsb50% (6)
- Bikol Reporter March 13 - 19, 2016 IssueDocument10 pagesBikol Reporter March 13 - 19, 2016 IssueBikol ReporterNo ratings yet
- DR Paul Harijanto - WS MALARIA-PIN PAPDI-19 PDFDocument33 pagesDR Paul Harijanto - WS MALARIA-PIN PAPDI-19 PDFMukhammadBurhanuddinNo ratings yet
- EAP Foundation What Is Ac WritingDocument6 pagesEAP Foundation What Is Ac WritingColin RobertsNo ratings yet
- An Approach To A Child With OedemaDocument14 pagesAn Approach To A Child With OedemaAdlina PutriantiNo ratings yet
- Narrative of Dry Run SimulationDocument2 pagesNarrative of Dry Run SimulationJhen SalamatNo ratings yet
- Tuberculosis: GlobalDocument75 pagesTuberculosis: GlobalNAILA NEVES DE JESUSNo ratings yet
- Antimony Gluconate-1Document13 pagesAntimony Gluconate-1humag143100% (3)
- Seminar 3 QuestionsDocument3 pagesSeminar 3 QuestionsWafaa AdamNo ratings yet
- Tarea 4 de Ingles 4 UNIVERSIDAD ABIERTA PARA ADULTOS UAPADocument6 pagesTarea 4 de Ingles 4 UNIVERSIDAD ABIERTA PARA ADULTOS UAPAAlexander Polanco50% (2)
- Rahu KetuDocument3 pagesRahu KetuMumbai BombayNo ratings yet