You might also like
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- Oral Wound Healing: Cell Biology and Clinical ManagementFrom EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaNo ratings yet
- Clinical Success in Resin Bonded Bridges PDFDocument7 pagesClinical Success in Resin Bonded Bridges PDFNajeeb UllahNo ratings yet
- Jurnal Mounting Articulator PDFDocument6 pagesJurnal Mounting Articulator PDFKhaleda ShafiraNo ratings yet
- Comparative Evaluation of The Mechanical Properties of Three Commercially Available Flexible Denture Base Materials - An in Vitro StudyDocument132 pagesComparative Evaluation of The Mechanical Properties of Three Commercially Available Flexible Denture Base Materials - An in Vitro StudySkAliHassanNo ratings yet
- Klasifikasi AramanyDocument7 pagesKlasifikasi AramanyErwin SutonoNo ratings yet
- Space RegainerDocument7 pagesSpace RegainerdelfNo ratings yet
- Prostho Vi - Slides 5 - Occlusal - ConsiderationsDocument83 pagesProstho Vi - Slides 5 - Occlusal - Considerationsبراءة أحمد السلاماتNo ratings yet
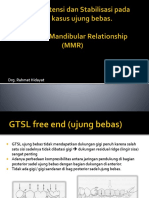
- Dok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRDocument53 pagesDok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRAditya ZulfikarNo ratings yet
- Porcelain Fused To Metal CrownsDocument5 pagesPorcelain Fused To Metal CrownsCitra Dwi PrastiwieNo ratings yet
- Jurnal Reading Bedah MulutDocument27 pagesJurnal Reading Bedah MulutArismunandar SosiloNo ratings yet
- Classification System For Full EdentulismDocument4 pagesClassification System For Full EdentulismmandakinimohanNo ratings yet
- IckDocument6 pagesIckbkprosthoNo ratings yet
- 14 - Perawatan Endodontic Gigi Molar Dengan Perforasi BifurkasiDocument5 pages14 - Perawatan Endodontic Gigi Molar Dengan Perforasi Bifurkasisarah hanifahNo ratings yet
- Section 1 Abrasive Produk EbookDocument16 pagesSection 1 Abrasive Produk EbookKurniawanNo ratings yet
- FINAL SplintingDocument46 pagesFINAL SplintingDilmohit SinghNo ratings yet
- Occlusal AdjustmentDocument11 pagesOcclusal Adjustmentpablo_elguezábalNo ratings yet
- Arch BarDocument28 pagesArch BarFachrul Latif DentistNo ratings yet
- Curve of SpeeDocument7 pagesCurve of SpeeKorina CallerosNo ratings yet
- Restorative Technique Selection in Class IV Direct Composite Restorations: A Simplified MethodDocument6 pagesRestorative Technique Selection in Class IV Direct Composite Restorations: A Simplified MethodCalisto GomesNo ratings yet
- By, Kavitha Shaji Paul 3 Yr B.D.SDocument33 pagesBy, Kavitha Shaji Paul 3 Yr B.D.SNino JohnNo ratings yet
- Rak Single DentureDocument48 pagesRak Single Denturerakes0No ratings yet
- Clinical Applications of Biodentine in Pediatric Dentistry A Review Ofliterature 2332 0702 1000179 PDFDocument6 pagesClinical Applications of Biodentine in Pediatric Dentistry A Review Ofliterature 2332 0702 1000179 PDFZita AprilliaNo ratings yet
- Modern DesignDocument50 pagesModern DesignasepNo ratings yet
- Bridge Indikasi & DesainDocument86 pagesBridge Indikasi & DesainFrieda Ayu PrihadiniNo ratings yet
- Section - 026 - Immediate DenturesDocument12 pagesSection - 026 - Immediate DenturesMuli Maroshi100% (1)
- Coronoplasty 2Document4 pagesCoronoplasty 2Befalia Aisarahmadani100% (1)
- SSCDocument10 pagesSSCYanuar MegaNo ratings yet
- Daftar Harga Kurnia Dental Laboratory Per Juli 2018Document2 pagesDaftar Harga Kurnia Dental Laboratory Per Juli 2018ferdyNo ratings yet
- Preparasi Gigi AbutmentDocument15 pagesPreparasi Gigi AbutmentFransiskus Xaverius DoddieNo ratings yet
- Acc Pain FauziDocument8 pagesAcc Pain FauziMuchlis Fauzi ENo ratings yet
- Dosen FKG Data Feb 2018Document9 pagesDosen FKG Data Feb 2018ayuasriyaniayuNo ratings yet
- UndercutsDocument4 pagesUndercutsokk12345No ratings yet
- Black Pigmentation in Primary Dentition Case Report and Literature ReviewDocument5 pagesBlack Pigmentation in Primary Dentition Case Report and Literature ReviewlaloNo ratings yet
- Space Regainers in Pediatric DentistryDocument6 pagesSpace Regainers in Pediatric DentistryFayiz SäbNo ratings yet
- Modified Bluegrass Appliance PDFDocument4 pagesModified Bluegrass Appliance PDFRenieKumalaNo ratings yet
- Occlusal TraumaDocument3 pagesOcclusal TraumaAbdullah SaleemNo ratings yet
- Tes TLMDocument16 pagesTes TLMAmelia RosyidaNo ratings yet
- Tetric N-CollectionDocument21 pagesTetric N-CollectionGustavo Pacheco0% (1)
- Adhesive Restorations, Centric Relation and The Dahl PrincipleDocument15 pagesAdhesive Restorations, Centric Relation and The Dahl PrincipleJorge RojasNo ratings yet
- 1.1 Endodontik: HealingDocument52 pages1.1 Endodontik: HealingARINA KHAQ100% (1)
- Cavity Preparation For Indirect RestorationsDocument7 pagesCavity Preparation For Indirect RestorationsAhmed M100% (1)
- Hidden CariesDocument10 pagesHidden Cariesyenni_windasariNo ratings yet
- Case Report Fissure SealantDocument8 pagesCase Report Fissure SealantrespikNo ratings yet
- Modified Pontic Design For Ridge DefectsDocument11 pagesModified Pontic Design For Ridge DefectsFaheemuddin MuhammadNo ratings yet
- Review Correlation Between Diabetes Mellitus and Residual Ridge Resorption PDFDocument3 pagesReview Correlation Between Diabetes Mellitus and Residual Ridge Resorption PDFInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Hemiseksi Akar Distal Molar Kedua Rahang BawahDocument5 pagesHemiseksi Akar Distal Molar Kedua Rahang BawahAhmad Willy AntonNo ratings yet
- Daftar Judul Jurnal Pedodonsia Gel IDocument4 pagesDaftar Judul Jurnal Pedodonsia Gel IRinaldi InalNo ratings yet
- Guided Tissue RegenerationDocument4 pagesGuided Tissue RegenerationNicoleta MarcuNo ratings yet
- Polishing Amalgam RestorationsDocument39 pagesPolishing Amalgam RestorationsMuad AbulohomNo ratings yet
- Immediate DentureDocument52 pagesImmediate Denturedkdinesh020No ratings yet
- Case Report - Complete Denture - 2Document4 pagesCase Report - Complete Denture - 2Astri Ggamjong Xiao LuNo ratings yet
- Scully 2016 PDFDocument14 pagesScully 2016 PDFDewi ZakiawatiNo ratings yet
- Emergency Dental Care: A Comprehensive Guide for Dental Patients: All About DentistryFrom EverandEmergency Dental Care: A Comprehensive Guide for Dental Patients: All About DentistryNo ratings yet
- Dentine Hypersensitivity: Developing a Person-centred Approach to Oral HealthFrom EverandDentine Hypersensitivity: Developing a Person-centred Approach to Oral HealthNo ratings yet
- AIPG 2004 (Dental)Document27 pagesAIPG 2004 (Dental)DENTALORG.COM100% (1)
- Dental GypsumsDocument2 pagesDental GypsumsAmr KassemNo ratings yet
- Retailer Wise 5 Days DataDocument14 pagesRetailer Wise 5 Days DataShilpa ShrivastavaNo ratings yet
- Agile ManifestoDocument22 pagesAgile ManifestoShilpa ShrivastavaNo ratings yet
- The Magical Number Seven, Plus or Minus TwoDocument4 pagesThe Magical Number Seven, Plus or Minus TwoVanya MaximovNo ratings yet
- GK Today 2016 General Sciences PDFDocument294 pagesGK Today 2016 General Sciences PDFHasan Shaikh100% (2)
- NCP - Ineffective Airway Clearance R/T Retained Secretions 2° BPNDocument1 pageNCP - Ineffective Airway Clearance R/T Retained Secretions 2° BPNCarl Elexer Cuyugan Ano100% (2)
- GPP in Tropical Ecosystems (Monteith, 1972)Document21 pagesGPP in Tropical Ecosystems (Monteith, 1972)Archis LikhitkarNo ratings yet
- Brainstem Medulla Pons MidbrainDocument3 pagesBrainstem Medulla Pons MidbrainAngela HabaradasNo ratings yet
- DEGLUTITIONDocument39 pagesDEGLUTITIONmamatha dNo ratings yet
- Arterial Lines Mark Hammerschmidt, RN FromDocument9 pagesArterial Lines Mark Hammerschmidt, RN FromMark Hammerschmidt100% (3)
- Biochem Rev Chap 8Document3 pagesBiochem Rev Chap 8Jacob PallorinaNo ratings yet
- Assessing Thorax LungsDocument20 pagesAssessing Thorax Lungskyla boncacasNo ratings yet
- The Trigeminal and Facial NervesDocument7 pagesThe Trigeminal and Facial NervesJose CastroNo ratings yet
- Wax and EstersDocument7 pagesWax and EstersPamela Mae UcabNo ratings yet
- Biology Exemplar ProblemsDocument5 pagesBiology Exemplar ProblemsAkshatha NayakNo ratings yet
- Peginesatide For Anemia in Patients With Chronic Kidney Disease Not Receiving DialysisDocument21 pagesPeginesatide For Anemia in Patients With Chronic Kidney Disease Not Receiving DialysisEdi Kurnawan TjhaiNo ratings yet
- Endoscopic InvestigationsDocument1 pageEndoscopic Investigationsgeorgeloto12No ratings yet
- Regional Sales Manager Medical Devices in Dallas FT Worth TX Resume James MooreDocument2 pagesRegional Sales Manager Medical Devices in Dallas FT Worth TX Resume James MooreJamesMoore2No ratings yet
- Bio Lab # 6Document5 pagesBio Lab # 6Cris SanchEzNo ratings yet
- Full PDFDocument399 pagesFull PDFTeresa Marie Yap CorderoNo ratings yet
- CBC ReportsDocument2 pagesCBC ReportsIbrar Hussain100% (1)
- Strength and HealthDocument37 pagesStrength and HealthhugocoutoNo ratings yet
- Apical Third and Its SignificanceDocument20 pagesApical Third and Its SignificanceBharath Ratnakaram100% (1)
- Protos, Meaning of The First Rank' or of PrimeDocument16 pagesProtos, Meaning of The First Rank' or of Primepinkish7_preciousNo ratings yet
- Chapter 2. Acute and Chronic InflammationDocument6 pagesChapter 2. Acute and Chronic InflammationWaseem Khan AfridiNo ratings yet
- A Quick Guide To Grand Practical Exam in ElectrotherapyDocument8 pagesA Quick Guide To Grand Practical Exam in ElectrotherapyJohnpeter EsporlasNo ratings yet
- Anaesthesia For Paediatric Robotic Assisted Thoracoscopic SurgeryDocument6 pagesAnaesthesia For Paediatric Robotic Assisted Thoracoscopic SurgeryPrabakaran ParameswaranNo ratings yet
- EHBADocument14 pagesEHBAJennifer DixonNo ratings yet
- 03 Yeast Metabolism PDFDocument12 pages03 Yeast Metabolism PDFMlopezNo ratings yet
- The Cervical & Thoracic Spine - Mechanical Diagnosis & Therapy - Vol 2Document288 pagesThe Cervical & Thoracic Spine - Mechanical Diagnosis & Therapy - Vol 2booksbearreading100% (6)
- Anaesthetic Drug Crib Sheet-8 PDFDocument1 pageAnaesthetic Drug Crib Sheet-8 PDFRicky Andhika Pratama100% (1)
- Protein Characterization/Purification: Dr. Kevin AhernDocument34 pagesProtein Characterization/Purification: Dr. Kevin AhernkelpachurpaNo ratings yet
- Nursing Review Exam Questions FUNDADocument10 pagesNursing Review Exam Questions FUNDAAlibasher MacalnasNo ratings yet