You might also like
- Maternal Health Nursing - 50 Item Without RatioDocument3 pagesMaternal Health Nursing - 50 Item Without RatioDennis Nabor Muñoz, RN,RMNo ratings yet
- Pedia W RationalesDocument43 pagesPedia W RationalesCamille BastonNo ratings yet
- My Reviewer On Funda Epaphras Joel T. MilitarDocument82 pagesMy Reviewer On Funda Epaphras Joel T. MilitarEpaphras Joel MilitarNo ratings yet
- Signs of LaborDocument40 pagesSigns of LaborDominicSavioNo ratings yet
- Legal Aspect Governing Disclosure of Health InformationDocument25 pagesLegal Aspect Governing Disclosure of Health InformationCLEMENT100% (5)
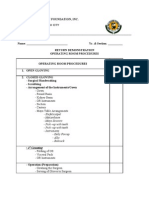
- Or Return Demo FinalDocument2 pagesOr Return Demo FinallemuelNo ratings yet
- Situation 1 - Mr. Ibarra Is Assigned To The Triage Area and While On Duty, He Assesses The Condition of Mrs. Simon WhoDocument52 pagesSituation 1 - Mr. Ibarra Is Assigned To The Triage Area and While On Duty, He Assesses The Condition of Mrs. Simon Whogerald_ichigoNo ratings yet
- Medical Surgical Nursing Understanding HemophiliaDocument2 pagesMedical Surgical Nursing Understanding HemophiliaChieChay DubNo ratings yet
- Universal Principles of NCMDocument43 pagesUniversal Principles of NCM+nella100% (1)
- Cemonc: Esmas, Lexi MCN 2 Le 1 1Document8 pagesCemonc: Esmas, Lexi MCN 2 Le 1 1EmpieNo ratings yet
- Breastfeeding and HivDocument30 pagesBreastfeeding and HivbxrbxrNo ratings yet
- Psychiatric Nursing (Notes) : Alcohol AbuseDocument88 pagesPsychiatric Nursing (Notes) : Alcohol AbuseJulie Ann ParaNo ratings yet
- Maternal and ChildDocument33 pagesMaternal and Childjosephine100% (1)
- NCLEX Practice Exam: Cardiovascular QuestionsDocument9 pagesNCLEX Practice Exam: Cardiovascular QuestionsYa Mei LiNo ratings yet
- Community Health Assessment of Rosario VillageDocument2 pagesCommunity Health Assessment of Rosario VillageCindy MariscotesNo ratings yet
- Power Git EndoDocument170 pagesPower Git Endoapi-3735995100% (1)
- Community Health Nursing ExamsDocument13 pagesCommunity Health Nursing ExamsAhrisJeannine EscuadroNo ratings yet
- CHNDocument38 pagesCHNLouie John AbilaNo ratings yet
- Sanitation Facilities and Waste DisposalDocument79 pagesSanitation Facilities and Waste DisposalKathy YoungNo ratings yet
- BulletsDocument14 pagesBulletsstuffednurseNo ratings yet
- Self Directive LearningDocument18 pagesSelf Directive Learningcrystal fate valdezNo ratings yet
- Assess, Classify, Treat and Follow Up a Sick ChildDocument33 pagesAssess, Classify, Treat and Follow Up a Sick Childrazorblades0012No ratings yet
- Leopold'S Maneuver: DefinitionDocument3 pagesLeopold'S Maneuver: DefinitionJyra Mae TaganasNo ratings yet
- Preoperative Surgical NursngDocument271 pagesPreoperative Surgical NursngPaw PawNo ratings yet
- HTTP://WWW - Aaroncyuntalan.com/newhandouts1/ Pediatric NursingDocument99 pagesHTTP://WWW - Aaroncyuntalan.com/newhandouts1/ Pediatric Nursingchelljynxie100% (2)
- RESPIRATORY SYSTEM Nclex Iloilo 4Document27 pagesRESPIRATORY SYSTEM Nclex Iloilo 4Barangay Centro SurNo ratings yet
- Hiatal HerniaDocument6 pagesHiatal HerniaElaine Jean UayanNo ratings yet
- Urinary EliminationDocument26 pagesUrinary EliminationyeshumasihNo ratings yet
- COPAR Vs CoM ORGDocument21 pagesCOPAR Vs CoM ORGAyaBasilioNo ratings yet
- Ob 100 RatioDocument13 pagesOb 100 RatioJUANJOSEFOXNo ratings yet
- Wound Care ChecklistDocument2 pagesWound Care ChecklistJay Lemuel BuenviajeNo ratings yet
- EP7 - ET Suctioning SlideshowDocument19 pagesEP7 - ET Suctioning SlideshowYashodhara Ghosh SenNo ratings yet
- University of Perpetual Help System DALTA: College of Radiologic TechnologyDocument2 pagesUniversity of Perpetual Help System DALTA: College of Radiologic TechnologyJynrose Kaye GulpanyNo ratings yet
- Integrated Management of Childhood Illness (IMCI) : Guide For Clinical PracticeDocument79 pagesIntegrated Management of Childhood Illness (IMCI) : Guide For Clinical PracticeCAREZAMBIA100% (1)
- NCM 101 (Continuation) Postpartal Period and PediatricsDocument29 pagesNCM 101 (Continuation) Postpartal Period and PediatricsAudi Kyle SaydovenNo ratings yet
- Scope of Nle1116aDocument413 pagesScope of Nle1116aericNo ratings yet
- Alterations in Nutrition and GastrointestinalDocument7 pagesAlterations in Nutrition and GastrointestinalChriszanie CruzNo ratings yet
- Expanded Program On ImmunizationDocument15 pagesExpanded Program On ImmunizationReygie MarsadaNo ratings yet
- Doh - Mental Health Gap Action ProgramDocument4 pagesDoh - Mental Health Gap Action ProgramCassey AnneNo ratings yet
- Eriksons Developmental StagesDocument1 pageEriksons Developmental StagesFilipino Nurses CentralNo ratings yet
- Doh MCNDocument14 pagesDoh MCNCbrc CebuNo ratings yet
- The Intrauterine Device: HealthDocument2 pagesThe Intrauterine Device: HealthApris Tesryanto LiufetoNo ratings yet
- Family Health AssessmentDocument23 pagesFamily Health AssessmentPatrick Poculan100% (1)
- COLORECTAL CANCER: SIGNS, STAGES, RISK FACTORS & TREATMENTDocument31 pagesCOLORECTAL CANCER: SIGNS, STAGES, RISK FACTORS & TREATMENTIrene RealinoNo ratings yet
- MCHN Reviewer 1Document24 pagesMCHN Reviewer 1Steam LcNo ratings yet
- Laws Affecting The Practice of Nursing in The PhilippinesDocument3 pagesLaws Affecting The Practice of Nursing in The Philippinessebo_Ü100% (1)
- Pediatric Nursing Student HandoutsDocument17 pagesPediatric Nursing Student HandoutsPaulAliboghaNo ratings yet
- Philippine NLE Board ExamDocument39 pagesPhilippine NLE Board ExamLloyd MelanaNo ratings yet
- Community Health Nursing Goals and FunctionsDocument15 pagesCommunity Health Nursing Goals and FunctionsFrancis Rafael PadillaNo ratings yet
- Medical Surgical Nurse Practice TestDocument4 pagesMedical Surgical Nurse Practice Testazazelshine0% (1)
- Idiopathic Thrombocytopenic Purpura (ITP)Document7 pagesIdiopathic Thrombocytopenic Purpura (ITP)Rizqka PertiwiNo ratings yet
- Nursing Bullets: Fundamentals of Nursing ReviewerDocument44 pagesNursing Bullets: Fundamentals of Nursing ReviewerErl DiamanteNo ratings yet
- June 2007-NPT 1 - RationaleDocument15 pagesJune 2007-NPT 1 - Rationaleяoxel яayмoи eитяeиaNo ratings yet
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- Rationale - Habon, CristineDocument21 pagesRationale - Habon, Cristinecha liNo ratings yet
- Um CareDocument15 pagesUm CareRose Anne Riotoc BarrientosNo ratings yet
- Obstetirc NursingDocument36 pagesObstetirc NursingGlenn Daryll SantosNo ratings yet
- Principles of Postpartum Nursing CareDocument2 pagesPrinciples of Postpartum Nursing CareZaire DylanNo ratings yet
- Geography of The BrainDocument1 pageGeography of The BrainmarieNo ratings yet
- Geography of The BrainDocument1 pageGeography of The BrainmarieNo ratings yet
- RNHeals AppformDocument1 pageRNHeals AppformmarieNo ratings yet
- Newborn PaDocument34 pagesNewborn PamarieNo ratings yet
- Drug Study1Document3 pagesDrug Study1marieNo ratings yet
- Ordinary QuotesDocument1 pageOrdinary QuotesmarieNo ratings yet
- MCN Print 3 NotesDocument1 pageMCN Print 3 NotesmarieNo ratings yet
- MCN Notes Print 1Document2 pagesMCN Notes Print 1marieNo ratings yet
- Inguinal Hernia With LabsDocument10 pagesInguinal Hernia With LabsmarieNo ratings yet
- Drug StudyDocument4 pagesDrug StudymarieNo ratings yet
- Psychia Review Notes (Incmplt)Document3 pagesPsychia Review Notes (Incmplt)marieNo ratings yet
- Meet The Piano (So Simple., Made Simple)Document5 pagesMeet The Piano (So Simple., Made Simple)marieNo ratings yet
- Drug StudyDocument5 pagesDrug Studymarie67% (3)
- Behavioral Therapy by Kurt LewinDocument6 pagesBehavioral Therapy by Kurt LewinmarieNo ratings yet
- Nursing Practice 1Document4 pagesNursing Practice 1marieNo ratings yet
- COPAR PREENTRY PHASE Preliminary Social InvestigationDocument3 pagesCOPAR PREENTRY PHASE Preliminary Social InvestigationmarieNo ratings yet
- Colostomy ProcedureDocument2 pagesColostomy Proceduremarie100% (2)
- Newborn PaDocument34 pagesNewborn Pamarie100% (2)
- 11 Core Competencies Part 1 To Part 2Document4 pages11 Core Competencies Part 1 To Part 2marie100% (2)
- China BrochureDocument2 pagesChina BrochuremarieNo ratings yet
- Founder: Categories Christianity Confucianism Buddhism Taoism Islam HinduismDocument3 pagesFounder: Categories Christianity Confucianism Buddhism Taoism Islam HinduismmarieNo ratings yet
- ECGDocument2 pagesECGmarie80% (5)
- The Aging Society: Its Effects On Health Care DeliveryDocument15 pagesThe Aging Society: Its Effects On Health Care Deliverymarie100% (2)
- Buddhism BrochureDocument3 pagesBuddhism Brochuremarie60% (10)
- Nasogastric Tube InsertionDocument3 pagesNasogastric Tube Insertionmarie100% (5)
- Administering An Enema EQUIPMENT Prepackaged Enema or Enema Container DisposableDocument3 pagesAdministering An Enema EQUIPMENT Prepackaged Enema or Enema Container Disposablemarie100% (2)
- Nursing Action Rationale Preparatory PhaseDocument6 pagesNursing Action Rationale Preparatory Phasemarie100% (2)
- Physiology of Aging 2005Document42 pagesPhysiology of Aging 2005marie100% (2)
- Nasogastric Tube FeedingDocument6 pagesNasogastric Tube Feedingmarie100% (5)
- Blood TransfusionDocument3 pagesBlood TransfusionmarieNo ratings yet
- Placental AbnormalitiesDocument7 pagesPlacental AbnormalitiesLrak SiaNo ratings yet
- AJOG Modelo Predictivo para Preeclampsia Nicolaides 2019Document13 pagesAJOG Modelo Predictivo para Preeclampsia Nicolaides 2019Ana PadillaNo ratings yet
- The Relationship Between Dietary Patterns and Nutritional Knowledge With The Nutritional Status of Bajo Tribe Pregnant Women in Duruka District, Muna RegencyDocument5 pagesThe Relationship Between Dietary Patterns and Nutritional Knowledge With The Nutritional Status of Bajo Tribe Pregnant Women in Duruka District, Muna RegencytreesNo ratings yet
- A GCE Biology 2805 01 January 2008 Question PaperDocument20 pagesA GCE Biology 2805 01 January 2008 Question PaperVeer RamloghunNo ratings yet
- Project On Flower v1.0Document10 pagesProject On Flower v1.0powerleader50% (2)
- Understanding PCOS in AdolescentsDocument14 pagesUnderstanding PCOS in AdolescentsJalajarani AridassNo ratings yet
- Squirting For DummiesDocument31 pagesSquirting For DummiesGustavoCalderin75% (4)
- Developmental Biology: GametogenesisDocument21 pagesDevelopmental Biology: GametogenesisTapan Kumar PalNo ratings yet
- JADWAL 8-10 JULI 2019Document12 pagesJADWAL 8-10 JULI 2019Hartanto LieNo ratings yet
- Exposed The Truth About Penis Enlargement Methods and DevicesDocument9 pagesExposed The Truth About Penis Enlargement Methods and DevicesCarl Cu100% (3)
- 3 Tissues in The Human Body 22864Document11 pages3 Tissues in The Human Body 22864Musharaf RehmanNo ratings yet
- Men Orr HagiaDocument15 pagesMen Orr HagiaJ SNo ratings yet
- SWCRM Sperm CryopreservationDocument2 pagesSWCRM Sperm CryopreservationVenkata Ramanan Dasu SubramanianNo ratings yet
- Revised Bioethics SyllabusDocument7 pagesRevised Bioethics SyllabuslouradelNo ratings yet
- Menstrual Health and Hygiene: Awareness and Communication in Rural AreasDocument7 pagesMenstrual Health and Hygiene: Awareness and Communication in Rural AreasAradhanaSinghNo ratings yet
- TestesDocument39 pagesTestesImadShaheen50% (2)
- MEOWS Guide Improves Maternity CareDocument7 pagesMEOWS Guide Improves Maternity CaredeviNo ratings yet
- Pi Low Lying Placenta 2007Document7 pagesPi Low Lying Placenta 2007Siti Asiah Abdul HalimNo ratings yet
- Vajikarana - Concept 1Document34 pagesVajikarana - Concept 1Raghu NaikNo ratings yet
- Estrous Cycle in The Bitch and QueenDocument9 pagesEstrous Cycle in The Bitch and QueenSandrine WoolcockNo ratings yet
- Intrapartum CareDocument65 pagesIntrapartum Caremarkus_danusantosoNo ratings yet
- Parasitology NotesDocument18 pagesParasitology NotesPrativa RajbhandariNo ratings yet
- NclexDocument4 pagesNclexihatetouNo ratings yet
- BIOC19 Midterm 3Document16 pagesBIOC19 Midterm 3idk manNo ratings yet
- Chorionic Villi Sampling: A Prenatal Genetic TestDocument35 pagesChorionic Villi Sampling: A Prenatal Genetic TestGomathi Gomu100% (1)
- Differences between asexual and sexual reproductionDocument2 pagesDifferences between asexual and sexual reproductionKristiane Reyes De VillaNo ratings yet
- Reproduction MCQsDocument2 pagesReproduction MCQssuriNo ratings yet
- Disorders of Puberty and GinekomastiaDocument20 pagesDisorders of Puberty and GinekomastiaMuthia ArsilNo ratings yet
- Internal and External Structure of ChickensDocument7 pagesInternal and External Structure of ChickensBerry PrinNo ratings yet
- Unit8 - GeneticsProblems - Assignment KeyDocument5 pagesUnit8 - GeneticsProblems - Assignment KeyJasmine KingNo ratings yet