You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Philippine Health Care Delivery System.Document7 pagesThe Philippine Health Care Delivery System.Mimi Lizada Bhatti100% (1)
- George Lakoff - Cognitive ModelsDocument20 pagesGeorge Lakoff - Cognitive ModelsSchecky100% (10)
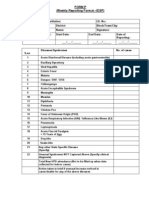
- IDSP P&L FormsDocument2 pagesIDSP P&L FormsKunal YadavNo ratings yet
- ThinkingPoints Chapter1Document7 pagesThinkingPoints Chapter1marklarNo ratings yet
- Mary Magdalene Be Author of The Fourth GospelDocument14 pagesMary Magdalene Be Author of The Fourth GospelWilliam MamudiNo ratings yet
- JokoBeck ThePoolsDocument3 pagesJokoBeck ThePoolsScheckyNo ratings yet
- Pema Chodron QuotesDocument2 pagesPema Chodron QuotesSchecky100% (1)
- Paulcuffee SierraleoneliberiaDocument1 pagePaulcuffee SierraleoneliberiaScheckyNo ratings yet
- Turning Toward PainDocument9 pagesTurning Toward PainScheckyNo ratings yet
- George Lakoff - The Contemporary Theory of MetaphorDocument46 pagesGeorge Lakoff - The Contemporary Theory of MetaphorAntonio Giovinazzo100% (1)
- Implications of Lipid Biology For The Pathogenesis of SchizophreniaDocument12 pagesImplications of Lipid Biology For The Pathogenesis of SchizophreniaScheckyNo ratings yet
- Selections From Paul JohnsonDocument5 pagesSelections From Paul JohnsonScheckyNo ratings yet
- HP March April BigDocument1 pageHP March April BigScheckyNo ratings yet
- HP Mayjune BigDocument1 pageHP Mayjune BigScheckyNo ratings yet
- Family LeaveDocument7 pagesFamily LeaveScheckyNo ratings yet
- Rhino TankDocument1 pageRhino TankScheckyNo ratings yet
- Holocaust Literacy LessonsDocument5 pagesHolocaust Literacy LessonsScheckyNo ratings yet
- George Lakoff - Metaphor, Morality & Politics, Or, Why Conservatives Have Left Liberals in The DustDocument22 pagesGeorge Lakoff - Metaphor, Morality & Politics, Or, Why Conservatives Have Left Liberals in The DustSchecky100% (5)
- George Lakoff - Framing The Issue - How Conservatives Use Language To Dominate Politics 2003.10.27Document5 pagesGeorge Lakoff - Framing The Issue - How Conservatives Use Language To Dominate Politics 2003.10.27ScheckyNo ratings yet
- George Lakoff - Metaphor, Morality & Politics, Or, Why Conservatives Have Left Liberals in The DustDocument22 pagesGeorge Lakoff - Metaphor, Morality & Politics, Or, Why Conservatives Have Left Liberals in The DustSchecky100% (5)
- George Lakoff - Metaphors of TerrorDocument13 pagesGeorge Lakoff - Metaphors of TerrorSchecky100% (1)
- George Lakoff - Mitecs - ReviewDocument15 pagesGeorge Lakoff - Mitecs - ReviewScheckyNo ratings yet
- George Lakoff - Don't Think of An Elephant - Know Your Values and Frame The DebateDocument142 pagesGeorge Lakoff - Don't Think of An Elephant - Know Your Values and Frame The DebateSchecky100% (4)
- In Uence of Gender On Social Outcome in SchizophreniaDocument7 pagesIn Uence of Gender On Social Outcome in SchizophreniaScheckyNo ratings yet
- George Lakoff - Metaphorical ThoughtDocument41 pagesGeorge Lakoff - Metaphorical ThoughtSchecky100% (2)
- George Lakoff - Framing The Debate It's All GOP 20070104Document2 pagesGeorge Lakoff - Framing The Debate It's All GOP 20070104ScheckyNo ratings yet
- CVPDPLANDocument8 pagesCVPDPLANScheckyNo ratings yet
- Cognitive Subprocesses and Schizophrenia. A. Reaction-Time DecompositionDocument10 pagesCognitive Subprocesses and Schizophrenia. A. Reaction-Time DecompositionScheckyNo ratings yet
- Challenge Day InformationDocument7 pagesChallenge Day InformationScheckyNo ratings yet
- California Losing LusterDocument4 pagesCalifornia Losing LusterScheckyNo ratings yet
- California Widening DivideDocument3 pagesCalifornia Widening DivideScheckyNo ratings yet
- Heli Electric Pallet Truck Cbd20 410 Parts Manual ZH enDocument22 pagesHeli Electric Pallet Truck Cbd20 410 Parts Manual ZH enpuhocuvy100% (34)
- Food Safety Officer Syllabus PSCDocument2 pagesFood Safety Officer Syllabus PSCA RahmanNo ratings yet
- DgfasliDocument9 pagesDgfasliAmitkumar SinghNo ratings yet
- Gynaecology Examination PRAVEENADocument15 pagesGynaecology Examination PRAVEENAPraveena MoganNo ratings yet
- CefuroximeDocument1 pageCefuroximehahahahaaaaaaaNo ratings yet
- Breastfeeding & Complementary Feeding: Basic PediatricsDocument13 pagesBreastfeeding & Complementary Feeding: Basic PediatricsChristian TayagNo ratings yet
- Expanded Program On ImmunizationDocument3 pagesExpanded Program On Immunizationapi-2658787986% (7)
- P-Form Weekly Idsp Alert - Week 09 BANASKANTHA PALANPURDocument11 pagesP-Form Weekly Idsp Alert - Week 09 BANASKANTHA PALANPURPankaj ModhNo ratings yet
- Legacy of Tuskegee Syphilis StudyDocument2 pagesLegacy of Tuskegee Syphilis StudyLcgessamanNo ratings yet
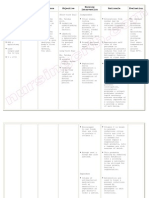
- Nursing Care Plan Risk For Uterine InfectionDocument4 pagesNursing Care Plan Risk For Uterine Infectionderic97% (30)
- Betty NewmanDocument23 pagesBetty NewmanDian ElvianaNo ratings yet
- Lenny NursithaDocument3 pagesLenny NursithaPERPUSTAKAAN SMA NEGERI 1 BATUJAYANo ratings yet
- VaccinesDocument29 pagesVaccinesCassandra EnriquezNo ratings yet
- NALFLEET 79112 Metal BrightenerDocument2 pagesNALFLEET 79112 Metal Brightenerdan antonNo ratings yet
- Preterm DeliveryDocument368 pagesPreterm DeliveryAbhishek VijayakumarNo ratings yet
- SNV - Baseline Study To Assess FSM of Residential PremisesDocument50 pagesSNV - Baseline Study To Assess FSM of Residential PremisesrupakhasanNo ratings yet
- Islcollective Worksheets Elementary A1 Preintermediate A2 Adults High School Reading Nouns Past Simple Tense Present Sim 12443234045615e4ee5608e3 21320522Document3 pagesIslcollective Worksheets Elementary A1 Preintermediate A2 Adults High School Reading Nouns Past Simple Tense Present Sim 12443234045615e4ee5608e3 21320522yrynuka yrysNo ratings yet
- BELLO DOCsDocument98 pagesBELLO DOCsPia Loraine BacongNo ratings yet
- Anticougulation in PregnancyDocument21 pagesAnticougulation in PregnancyLubna AliNo ratings yet
- Fiji - Greater Suva Urban ProfileDocument20 pagesFiji - Greater Suva Urban ProfileUnited Nations Human Settlements Programme (UN-HABITAT)No ratings yet
- Bashh PidDocument26 pagesBashh PidMarNo ratings yet
- Placement Hours Log TemplateDocument15 pagesPlacement Hours Log TemplateGareth McKnight100% (1)
- Incubation-Ranges Food SafetyDocument2 pagesIncubation-Ranges Food SafetyIngrid WaspodoNo ratings yet
- Vaginal Douching Among LatinasDocument9 pagesVaginal Douching Among LatinasSebastian Posada0% (1)
- Asuhan Keperawatan Pasien Dengan Sepsis: Ns. Anastasia Hardyati., M.Kep., Sp. KMBDocument17 pagesAsuhan Keperawatan Pasien Dengan Sepsis: Ns. Anastasia Hardyati., M.Kep., Sp. KMBchika wahyu sasqiautamiNo ratings yet
- Aruba BirreriaDocument1 pageAruba BirreriaBiagio SeniseNo ratings yet
- Katalog 27 September 2021Document28 pagesKatalog 27 September 2021Rafael BagusNo ratings yet
- Histeria Por Vacunación Mass Psychogenic Illness After Vaccination 2003Document6 pagesHisteria Por Vacunación Mass Psychogenic Illness After Vaccination 2003Oscar Alejandro Cardenas QuinteroNo ratings yet