You might also like
- What Are Your Million Dollar Questions?Document12 pagesWhat Are Your Million Dollar Questions?Pravin Prathip JNo ratings yet
- 0verview of Dental ImplantologyDocument70 pages0verview of Dental ImplantologyPravin Prathip JNo ratings yet
- Present Anything FrameworkDocument11 pagesPresent Anything FrameworkPravin Prathip JNo ratings yet
- Dental Practice Management BootcampDocument12 pagesDental Practice Management BootcampPravin Prathip JNo ratings yet
- 12 Best Questions To AskDocument117 pages12 Best Questions To AskhutsupNo ratings yet
- What Is Seo?: The Introductory Guide To Search Engine Optimization in 2017Document57 pagesWhat Is Seo?: The Introductory Guide To Search Engine Optimization in 2017Pravin Prathip J100% (1)
- Financial Forecasting For Serious-Minded Entrepreneurs (And Cfos)Document43 pagesFinancial Forecasting For Serious-Minded Entrepreneurs (And Cfos)Pravin Prathip JNo ratings yet
- Endodontics: For General PracticeDocument10 pagesEndodontics: For General PracticePravin Prathip JNo ratings yet
- 7 Steps To A Complete Dental Practice Sales & Marketing PlanDocument15 pages7 Steps To A Complete Dental Practice Sales & Marketing PlanPravin Prathip JNo ratings yet
- All On Four Dental Implant Options ExplainedDocument13 pagesAll On Four Dental Implant Options ExplainedPravin Prathip J100% (2)
- Dealing With Difficult People Free ReportDocument20 pagesDealing With Difficult People Free ReportJuan Luis GarvíaNo ratings yet
- BPS+ +the+Biofunctional+Prosthetic+SystemDocument20 pagesBPS+ +the+Biofunctional+Prosthetic+SystemPravin Prathip JNo ratings yet
- Endo Broucher Min FRDocument11 pagesEndo Broucher Min FRPravin Prathip JNo ratings yet
- Birth Certificate 2013 10 130 001682 0Document1 pageBirth Certificate 2013 10 130 001682 0Pravin Prathip JNo ratings yet
- Being Customer CentricDocument54 pagesBeing Customer CentricPravin Prathip JNo ratings yet
- A Clinical Review of The MBT™ Versatile+ ApplianceDocument32 pagesA Clinical Review of The MBT™ Versatile+ ApplianceKurt Krings0% (2)
- An Endo Revolution: With Only 3 Instruments!Document20 pagesAn Endo Revolution: With Only 3 Instruments!Pravin Prathip JNo ratings yet
- Diagnosis in EndodonticsDocument44 pagesDiagnosis in EndodonticsPravin Prathip JNo ratings yet
- Oral BDocument1 pageOral BPravin Prathip JNo ratings yet
- Treatment of Class II MalocclusionsDocument148 pagesTreatment of Class II MalocclusionsRenu Ann Mathew100% (2)
- Ihde Immediate Loading Info Ver2 enDocument22 pagesIhde Immediate Loading Info Ver2 enPravin Prathip J100% (1)
- Treatment of Class II MalocclusionsDocument148 pagesTreatment of Class II MalocclusionsRenu Ann Mathew100% (2)
- Canine RetractionDocument12 pagesCanine RetractionPravin Prathip JNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Space Control in Mixed Dentition - Space MaintaineDocument8 pagesSpace Control in Mixed Dentition - Space MaintaineamarakanyaNo ratings yet
- Dental Material MCQ Test Bank Chapter 011Document16 pagesDental Material MCQ Test Bank Chapter 011Táláát Älsurori100% (1)
- JCThree-dimensional Evaluation ofDocument26 pagesJCThree-dimensional Evaluation ofRohini TondaNo ratings yet
- Dental Ortho Management Software 1234Document13 pagesDental Ortho Management Software 1234RoyNo ratings yet
- 3.retention RelapseDocument40 pages3.retention RelapseMohamed Yosef Morad100% (1)
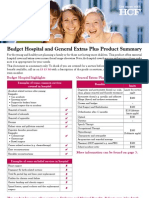
- Budget Hospital and General Extras Plus Product SummaryDocument4 pagesBudget Hospital and General Extras Plus Product SummaryJames SandersNo ratings yet
- New Concepts in Orthodontics, Occlusion and TMJ DysfunctionDocument8 pagesNew Concepts in Orthodontics, Occlusion and TMJ DysfunctionsorcNo ratings yet
- A To Z Orthodontics Vol 11 Functional Orthodontic AppliancesDocument22 pagesA To Z Orthodontics Vol 11 Functional Orthodontic AppliancesNisa Ulil AmriNo ratings yet
- Hevesi J. - Ortho - II.semester-4.week-2.lectureDocument30 pagesHevesi J. - Ortho - II.semester-4.week-2.lectureYaser JasNo ratings yet
- Ron Greenspan DDS - Braces 101Document10 pagesRon Greenspan DDS - Braces 101Ron Greenspan DDSNo ratings yet
- Orthodontics DClinDentDocument10 pagesOrthodontics DClinDentmubthasimimdadNo ratings yet
- SAQs For Dentistry, Third Edition 2015 PDFDocument651 pagesSAQs For Dentistry, Third Edition 2015 PDFDdot Dashene50% (2)
- Management of Skeletal Class II Deep BiteDocument5 pagesManagement of Skeletal Class II Deep BitewindyNo ratings yet
- Wedge Effect 2 PDFDocument7 pagesWedge Effect 2 PDFrohitNo ratings yet
- Retention and RelapseDocument92 pagesRetention and RelapseBimalKrishna100% (1)
- Forces and Moments Generated by Simon Et Al-Prot.20420449Document9 pagesForces and Moments Generated by Simon Et Al-Prot.20420449GhazwanNo ratings yet
- IJOI Vol43 DR - Anghileri ANG TechniqueDocument5 pagesIJOI Vol43 DR - Anghileri ANG TechniqueMatias AnghileriNo ratings yet
- Temporomandibular DisordersDocument45 pagesTemporomandibular DisordersMohsin HabibNo ratings yet
- Modified Precision Lingual Bonding Technique - A Step-Wise Approach With Torque Angulation Device-Bracket Positioning DeviceDocument5 pagesModified Precision Lingual Bonding Technique - A Step-Wise Approach With Torque Angulation Device-Bracket Positioning Devicesparkle dentalNo ratings yet
- New Table To Guide Bracket PlacementDocument4 pagesNew Table To Guide Bracket PlacementDr. Tomas Castellanos100% (2)
- NEET-MDS 2019 Seat Position SummaryDocument3 pagesNEET-MDS 2019 Seat Position SummaryNikhil BhandariNo ratings yet
- Bina Taar Tedhe Medhe Dant Sidhe Karne Ke Aasan Upay Hindi MeinDocument3 pagesBina Taar Tedhe Medhe Dant Sidhe Karne Ke Aasan Upay Hindi MeinGovindNo ratings yet
- Color Atlas of Dental Medicine Orthodontic Diagnosis PDFDocument2 pagesColor Atlas of Dental Medicine Orthodontic Diagnosis PDFMaria0% (2)
- Vertical Discrepancies and Their TreatmentDocument4 pagesVertical Discrepancies and Their TreatmentKajal Panchal19951995No ratings yet
- Dr. Emerita Birgit ThilanderDocument34 pagesDr. Emerita Birgit Thilandertanmayi minniNo ratings yet
- 5 Abstrak Myobrace - Harmawaty HamsirDocument1 page5 Abstrak Myobrace - Harmawaty HamsirjadeNo ratings yet
- Literature Review of Amelogenesis Imperfecta With Case ReportDocument6 pagesLiterature Review of Amelogenesis Imperfecta With Case Reportc5t9rejgNo ratings yet
- Elastic Activator For Treatment of Openbite Stellzig1999Document5 pagesElastic Activator For Treatment of Openbite Stellzig1999Thendral DevanathanNo ratings yet
- Changes in The Curve of SpeeDocument8 pagesChanges in The Curve of SpeeharpsychordNo ratings yet
- The Journey From The Past To The FutureDocument2 pagesThe Journey From The Past To The FutureplsssssNo ratings yet