You might also like
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- CS61A Notes 9 - Now The Mutants Attack (v1.1)Document5 pagesCS61A Notes 9 - Now The Mutants Attack (v1.1)studboyNo ratings yet
- Mortgage App Form 1003Document5 pagesMortgage App Form 1003api-305651288No ratings yet
- Tech Dev ChinaDocument29 pagesTech Dev ChinastudboyNo ratings yet
- Agile Life CycleDocument41 pagesAgile Life Cyclestudboy100% (2)
- IPOwnershipDocument16 pagesIPOwnershipstudboyNo ratings yet
- Orders of GrowthDocument8 pagesOrders of GrowthstudboyNo ratings yet
- Decode Your LicenseDocument9 pagesDecode Your Licensestudboy100% (4)
- IPChinaDocument28 pagesIPChinastudboyNo ratings yet
- CS61A Notes 03 - Lists: Chongyang Wang, Courtesy of Chung Wu and Evan ChouDocument3 pagesCS61A Notes 03 - Lists: Chongyang Wang, Courtesy of Chung Wu and Evan ChoustudboyNo ratings yet
- Openvera/Rvm To Systemverilog/Vmm Conversion: How To Avoid Death by A Thousand Cuts'Document28 pagesOpenvera/Rvm To Systemverilog/Vmm Conversion: How To Avoid Death by A Thousand Cuts'studboy100% (2)
- Flipflops AnswersDocument6 pagesFlipflops AnswersstudboyNo ratings yet
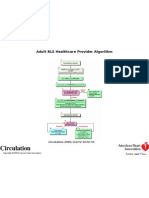
- Circulation Aha v112 I24 Suppl pIV-19 FIG2Document1 pageCirculation Aha v112 I24 Suppl pIV-19 FIG2studboyNo ratings yet
- SMChart MicroprogramDocument20 pagesSMChart MicroprogramstudboyNo ratings yet
- Implication AnswersDocument9 pagesImplication AnswersstudboyNo ratings yet
- FSM AnswersDocument6 pagesFSM AnswersstudboyNo ratings yet
- Chap. 15: Reduction of State Tables/ State AssignmentDocument64 pagesChap. 15: Reduction of State Tables/ State AssignmentstudboyNo ratings yet
- Parapro Test Study GuideDocument51 pagesParapro Test Study GuidestudboyNo ratings yet
- Fremont Union School District MapDocument1 pageFremont Union School District MapstudboyNo ratings yet
- Five Strategies For Marketing in Tough TimesDocument67 pagesFive Strategies For Marketing in Tough TimesstudboyNo ratings yet
- Gazettesep 07Document23 pagesGazettesep 07studboyNo ratings yet
- Gazettejan 08Document16 pagesGazettejan 08studboyNo ratings yet
- Gazettemay 08Document17 pagesGazettemay 08studboyNo ratings yet
- Saratoga School District MapDocument1 pageSaratoga School District MapstudboyNo ratings yet
- How To Present Effectively Online: An Osterman Research White Paper Prepared For Citrix SystemsDocument9 pagesHow To Present Effectively Online: An Osterman Research White Paper Prepared For Citrix Systemsstudboy100% (1)
- Business Intelligence PlaybookDocument32 pagesBusiness Intelligence Playbookstudboy100% (4)
- Hiv HandbookDocument78 pagesHiv HandbookstudboyNo ratings yet
- Nosmoking RentalsDocument3 pagesNosmoking RentalsstudboyNo ratings yet
- MultivitaminguideDocument18 pagesMultivitaminguidestudboy100% (3)
- Healthymouth HealthysexDocument20 pagesHealthymouth HealthysexstudboyNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
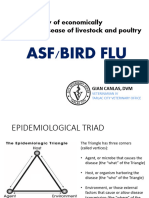
- Asf AiDocument59 pagesAsf AiAndrew FinoNo ratings yet
- Lessons from Recent Biosafety Incidents in the USDocument5 pagesLessons from Recent Biosafety Incidents in the USSANTIAGO HARVEY BENAVIDES RINCONNo ratings yet
- Mep Cover Infected - Indd 1 19/10/11 12:12:38Document32 pagesMep Cover Infected - Indd 1 19/10/11 12:12:38ZMGNo ratings yet
- Ethiopia Poultry Sector Overview for HPAI ResearchDocument36 pagesEthiopia Poultry Sector Overview for HPAI ResearchTade Gashaw0% (1)
- Week 5 Past Perfect Practice 2Document4 pagesWeek 5 Past Perfect Practice 2Soldjair Mantari SotoNo ratings yet
- Hannoun 2013Document10 pagesHannoun 2013bilou hertNo ratings yet
- CM UVC Certificate BacteriaDocument23 pagesCM UVC Certificate BacteriaFateh SinghNo ratings yet
- Academic and Professional Language SkillsDocument2 pagesAcademic and Professional Language Skillscherish mae oconNo ratings yet
- 1918 Flu Pandemic and the Role of FeverDocument7 pages1918 Flu Pandemic and the Role of Feverhhelp12255No ratings yet
- AHCC - Woodlands Patients GuideDocument80 pagesAHCC - Woodlands Patients GuidecrisperezNo ratings yet
- Bürgermeister, Jane. Evidence of The Use-Of Pandemic Flu To Depopulate USADocument134 pagesBürgermeister, Jane. Evidence of The Use-Of Pandemic Flu To Depopulate USASeverino P. CrispinNo ratings yet
- Mid Xii IpsDocument12 pagesMid Xii IpsEttyMarini Panggabean 11No ratings yet
- Influenza (The Flu) : Ain Shams UniversityDocument53 pagesInfluenza (The Flu) : Ain Shams UniversityfouadNo ratings yet
- Scope of ImmunologyDocument6 pagesScope of ImmunologySulove Koirala100% (2)
- H5N1 EngDocument8 pagesH5N1 EngHường ĐỗNo ratings yet
- IELTS General Training - Reading Comprehension Passage I: Questions 1-6Document14 pagesIELTS General Training - Reading Comprehension Passage I: Questions 1-6Bitan BanerjeeNo ratings yet
- Kaisa Study Final Paper Super FinalDocument114 pagesKaisa Study Final Paper Super FinalEunice RiveraNo ratings yet
- (Hans Zinsser, 1934 Quoted in Murphy 1994)Document43 pages(Hans Zinsser, 1934 Quoted in Murphy 1994)Saad MotawéaNo ratings yet
- Zlib - Pub How To Raise Poultry Everything You Need To KnowDocument178 pagesZlib - Pub How To Raise Poultry Everything You Need To KnowMarco VazquezNo ratings yet
- Oet R Floors RobbDocument22 pagesOet R Floors RobbKrishna VidhuriNo ratings yet
- Cloze TestDocument17 pagesCloze TestPayong Charernwisetsuk100% (2)
- Disease Emergence and Resurgence: The Wildlife-Human ConnectionDocument402 pagesDisease Emergence and Resurgence: The Wildlife-Human ConnectionMaíra100% (1)
- (Current Topics in Microbiology and Immunology 386) Michael B. A. Oldstone, Richard W. Compans (Eds.) - Influenza Pathogenesis and Control - Volume II (2015, Springer International Publishing)Document478 pages(Current Topics in Microbiology and Immunology 386) Michael B. A. Oldstone, Richard W. Compans (Eds.) - Influenza Pathogenesis and Control - Volume II (2015, Springer International Publishing)Wenny OktavianiNo ratings yet
- Eggcyclopedia Fifth Edition PDFDocument94 pagesEggcyclopedia Fifth Edition PDFKelvin MuzaNo ratings yet
- COVID-19 and The Wuhan Institute of Virology - GOP House Intel ReportDocument21 pagesCOVID-19 and The Wuhan Institute of Virology - GOP House Intel ReportAndy Belt50% (2)
- Bird FluDocument3 pagesBird FludocspaNo ratings yet
- Radiología Infecciones Tracto InferiorDocument26 pagesRadiología Infecciones Tracto InferioraleNo ratings yet
- Indian software outsourcing productivity due to strategic approachDocument8 pagesIndian software outsourcing productivity due to strategic approachVarshith_Reddy_7917No ratings yet
- Final Patch Update File - Michigan7 2017 BFHHRDocument637 pagesFinal Patch Update File - Michigan7 2017 BFHHRJeffrey WIlliamsNo ratings yet
- H5N1 FAQs: Bird Flu Questions AnsweredDocument3 pagesH5N1 FAQs: Bird Flu Questions AnsweredFiera RiandiniNo ratings yet