You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Strategic PlanDocument84 pagesStrategic PlanAurutchat VichaiditNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hematocrit and Hemoglobin DeterminationDocument32 pagesHematocrit and Hemoglobin DeterminationCeliz HilarioNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- State of The Air 2017Document164 pagesState of The Air 2017LancasterOnlineNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Healthmedicinet I 2017 3Document667 pagesHealthmedicinet I 2017 3tuni santeNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hepatitis BDocument12 pagesHepatitis BEmicar TecNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- MCN Lab WRDocument101 pagesMCN Lab WRMaui TabuzoNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Gastrointestinal Malignancies - New Innovative Diagnostics and Treatment PDFDocument712 pagesGastrointestinal Malignancies - New Innovative Diagnostics and Treatment PDFsun sealNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Lilium Tigrinum: Niki Taylor Lic. ISH IS HomDocument8 pagesLilium Tigrinum: Niki Taylor Lic. ISH IS HomNiki Taylor Lic ISH IS HOM100% (1)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Herpetiform Pemphigus: Courtesy, Ronald P Rapini, MDDocument1 pageHerpetiform Pemphigus: Courtesy, Ronald P Rapini, MDCristian QuitoNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Word Perioperative NursingDocument19 pagesWord Perioperative NursingGerald Resubal Oriña100% (1)
- Practical Radiotherapy PlanningDocument477 pagesPractical Radiotherapy PlanningZoran Mirkov100% (7)
- Step 2 CK QuestionsDocument8 pagesStep 2 CK QuestionsIrfan Majeed50% (2)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- 2.radiation Biology Q & ADocument7 pages2.radiation Biology Q & AdrpnnreddyNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Chapman's Reflexes and Modern Clinical ApplicationsDocument94 pagesChapman's Reflexes and Modern Clinical ApplicationsYuldash100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Newly Diagnosed GlioblastomaDocument30 pagesNewly Diagnosed GlioblastomaJubairNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Annexure - A Incident Assessment Risk MatrixDocument4 pagesAnnexure - A Incident Assessment Risk MatrixDilshad aliNo ratings yet
- Ozone Layer ProjectDocument27 pagesOzone Layer Project123456jinu0% (1)
- Sample Questions For HAAD Prometric and DHA For NursesDocument46 pagesSample Questions For HAAD Prometric and DHA For NursesJaezelle Ella Sabale100% (4)
- 13 Suppl1Document31 pages13 Suppl1VinodNo ratings yet
- Jco 22 02347Document11 pagesJco 22 02347Quang Thái NguyễnNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Aloe JuiceDocument12 pagesAloe JuiceAloe JuiceNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- PLCO Cancer Screening Trial Medication QuestionnaireDocument3 pagesPLCO Cancer Screening Trial Medication QuestionnaireGeede AlfonsoNo ratings yet
- Gentics PDFDocument7 pagesGentics PDFHarpreet KaurNo ratings yet
- BreastDocument8 pagesBreastNada MuchNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- 2.High-Resolution CT of The Lung EDITIA A-3-A.Document736 pages2.High-Resolution CT of The Lung EDITIA A-3-A.RamonataleNo ratings yet
- Contaminarea Cu MelaninaDocument8 pagesContaminarea Cu Melaninadiana fenichiuNo ratings yet
- Enlarged Peripheral Nerves On LeprosyDocument6 pagesEnlarged Peripheral Nerves On LeprosyGarrett SimpsonNo ratings yet
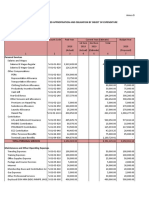
- Programmed Appropriation and Obligation by Object of ExpenditureDocument7 pagesProgrammed Appropriation and Obligation by Object of ExpenditureKristin Villaseñor-MercadoNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Lista de Lucrari 3Document30 pagesLista de Lucrari 3Anonymous 0epuGwQTJNo ratings yet
- Lsab KitDocument9 pagesLsab KitnutjabberNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)