You might also like
- Skin TractionDocument10 pagesSkin Tractionpritinez2516100% (1)
- Paranasal Sinus Cancer A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandParanasal Sinus Cancer A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Assessing The Ear and HearingDocument32 pagesAssessing The Ear and HearingArlyn Mendenilla0% (1)
- Unit 10 Activity & ExerciseDocument110 pagesUnit 10 Activity & ExerciseAshaNo ratings yet
- BCLS AclsDocument27 pagesBCLS AclsJanmichael FeliscuzoNo ratings yet
- Patient Positioning: Complete Guide For MidwivesDocument12 pagesPatient Positioning: Complete Guide For MidwivesRohlen BaguioNo ratings yet
- 17 Enteral and Parenteral NutritionDocument47 pages17 Enteral and Parenteral NutritionKathleen AngNo ratings yet
- Nursing Skills ChecklistDocument6 pagesNursing Skills Checklistapi-433883631No ratings yet
- Using Mechanical Aids For WalkinDocument38 pagesUsing Mechanical Aids For Walkinshannon c. lewisNo ratings yet
- ColostomyDocument4 pagesColostomyleslie_macasaetNo ratings yet
- Ambulating A PatientDocument5 pagesAmbulating A PatientSushmaNo ratings yet
- Gastric LavageDocument15 pagesGastric LavageEm BelandoNo ratings yet
- MyelographyDocument5 pagesMyelographyYamikaze MinatoNo ratings yet
- Promoting Nutrition (Enteral Nutrition)Document51 pagesPromoting Nutrition (Enteral Nutrition)Yayin Pestaño100% (1)
- HYDROCEPHALUSDocument63 pagesHYDROCEPHALUSAjeng Aristiany Rahawarin100% (2)
- Pre Op BabyDocument3 pagesPre Op BabyJmarie Brillantes PopiocoNo ratings yet
- Care For Patient With ColostomyDocument4 pagesCare For Patient With ColostomyJoseph C. CanielNo ratings yet
- TractionDocument3 pagesTractionEmmanuel Chris ArcayNo ratings yet
- CP - SoapieDocument2 pagesCP - SoapieNikki GalveNo ratings yet
- HSU 100-1 Choking and Other Conditions - Lecture 4Document84 pagesHSU 100-1 Choking and Other Conditions - Lecture 4Nixi MbuthiaNo ratings yet
- Draping The Operative ClientDocument7 pagesDraping The Operative ClientZIAN LABADIANo ratings yet
- ColostomyDocument13 pagesColostomyKetali JambhavdekarNo ratings yet
- Linear Arrangements of DR InstrumentsDocument42 pagesLinear Arrangements of DR Instrumentsxxegyzz100% (1)
- The Balanced Skeletal TractionDocument1 pageThe Balanced Skeletal TractionGemarie Adarlo CastilloNo ratings yet
- Physical Examination Instruments Audioscope - Used To Screen Patients Laryngeal Mirror - Used To Exam TheDocument8 pagesPhysical Examination Instruments Audioscope - Used To Screen Patients Laryngeal Mirror - Used To Exam TheSherish Millen CadayNo ratings yet
- Care of Patient With: Chest DrainageDocument29 pagesCare of Patient With: Chest DrainageMSc. PreviousNo ratings yet
- Urinary CatheterizationDocument2 pagesUrinary CatheterizationFains YdbwidNo ratings yet
- Fracture (Cast Care)Document6 pagesFracture (Cast Care)Vane UcatNo ratings yet
- Tracheostomy CareDocument40 pagesTracheostomy CareSreelekhaNo ratings yet
- Checklist For Bandage ApplicationDocument2 pagesChecklist For Bandage ApplicationAngelo AbiganiaNo ratings yet
- Tracheostomy CareDocument10 pagesTracheostomy CareSharifa Al AmerNo ratings yet
- Colostomy IrrigationDocument2 pagesColostomy IrrigationAudreySalvadorNo ratings yet
- DialysisDocument3 pagesDialysisSarah BenjaminNo ratings yet
- Aseptic TechniqueDocument7 pagesAseptic TechniqueRochele Buenavista- BuenaventuraNo ratings yet
- Vijendra Kumar: Compiled byDocument15 pagesVijendra Kumar: Compiled byvijendrakumarsahuNo ratings yet
- NCMB312 RLE OR Instrumentation Sutures Principles of Aseptic Techniques PDFDocument70 pagesNCMB312 RLE OR Instrumentation Sutures Principles of Aseptic Techniques PDFwokorow100% (1)
- Surgical Instruments RevisedDocument62 pagesSurgical Instruments RevisedDennis James BartolomeNo ratings yet
- Skin PreparationDocument3 pagesSkin Preparationmckulit_joey100% (2)
- OstomyDocument22 pagesOstomyJosiah VillacampaNo ratings yet
- Positioning and Draping The PatientDocument4 pagesPositioning and Draping The PatientNazire Luis Colita YandugNo ratings yet
- SinusitisDocument37 pagesSinusitismalathiNo ratings yet
- TAHBSODocument14 pagesTAHBSODafny CzarinaNo ratings yet
- Colostomy Care ChecklistDocument5 pagesColostomy Care ChecklistLynette JavaNo ratings yet
- ThyroidectomyDocument3 pagesThyroidectomyDomingo Trajada Jr.No ratings yet
- Ear DisordersDocument7 pagesEar DisordersGéorel John Colonia GoteraNo ratings yet
- ChockingDocument29 pagesChockingNoor A. ZakiNo ratings yet
- Fundal Height MeasurementDocument4 pagesFundal Height MeasurementChanta MaharjanNo ratings yet
- Ostomy Care: Esther Hattler, BS, RN, WCCDocument51 pagesOstomy Care: Esther Hattler, BS, RN, WCCAnita TermasNo ratings yet
- Ostomies: LessonDocument21 pagesOstomies: Lessonlovelykiss100% (1)
- Shock Concept MapDocument2 pagesShock Concept MapElizabeth GarretsonNo ratings yet
- Assessment:: Breast & AxillaeDocument96 pagesAssessment:: Breast & Axillaeafreenbegum-0502No ratings yet
- BIOPSYDocument8 pagesBIOPSYASHLEY DAWN BUENAFENo ratings yet
- Perioperative NursingDocument13 pagesPerioperative NursingTobiDaNo ratings yet
- CRUTCHESDocument35 pagesCRUTCHESBebing CostinianoNo ratings yet
- Cricothyroidotomy and Needle CricothyrotomyDocument10 pagesCricothyroidotomy and Needle CricothyrotomyDANDYNo ratings yet
- Operating Room InstrumentsDocument8 pagesOperating Room InstrumentsVictoria Castillo TamayoNo ratings yet
- Random Blood Sugar Estimation and Its SignificanceDocument11 pagesRandom Blood Sugar Estimation and Its Significanceapi-38237850% (1)
- Funda Rle Bed MakingDocument4 pagesFunda Rle Bed MakingIvan MaximusNo ratings yet
- Sense: Pietro PaoliniDocument34 pagesSense: Pietro PaolinisameshNo ratings yet
- Biomechanics of Knee JointDocument123 pagesBiomechanics of Knee JointSIBASIS PATTANAYAKNo ratings yet
- Histo NervousDocument20 pagesHisto NervousALESSANDRA CELINo ratings yet
- Chapter 6 Skeletal SystemDocument5 pagesChapter 6 Skeletal SystemCriscia Lene OlatNo ratings yet
- Manual Stretching TechniquesDocument26 pagesManual Stretching TechniquesjovisaroNo ratings yet
- Abc of EmgDocument61 pagesAbc of EmgJames WatanabeNo ratings yet
- Operative Treatment of Elbow Injuries PDFDocument169 pagesOperative Treatment of Elbow Injuries PDFBogdan SerbanNo ratings yet
- RBM 2530 - Tutorial 2 - Neuropathology-2011Document6 pagesRBM 2530 - Tutorial 2 - Neuropathology-2011Lina TanNo ratings yet
- DXA PRIMUSم الصادقDocument3 pagesDXA PRIMUSم الصادقBahaa Aldeen FadhilNo ratings yet
- Mcqs Nervuos SystemDocument4 pagesMcqs Nervuos Systemaslam jan100% (2)
- Sci 9 Q1 Module 1Document22 pagesSci 9 Q1 Module 1John Merby GonzalesNo ratings yet
- Beginner Sheiko Training ProgramsDocument52 pagesBeginner Sheiko Training ProgramsRyan PanNo ratings yet
- New Space Analysis 2021-2022Document23 pagesNew Space Analysis 2021-2022AseelNo ratings yet
- Pemeriksaan AbdomenDocument212 pagesPemeriksaan Abdomentamara hanna bocanNo ratings yet
- Medical Surgical Nursing 1Document43 pagesMedical Surgical Nursing 1Tifanny Shaine Tomas100% (2)
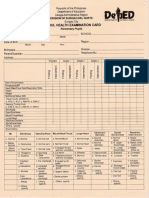
- School Health Examination Card For ElementaryDocument2 pagesSchool Health Examination Card For ElementaryWilma Villanueva86% (21)
- FSHNACritiqueandReappraisal PdfwiththreetablesDocument73 pagesFSHNACritiqueandReappraisal PdfwiththreetablesPhanQuangHuyNo ratings yet
- Thyroid Profile: Test Report Mr. Jogi Reddy N 50 Years / Male 230120006631Document1 pageThyroid Profile: Test Report Mr. Jogi Reddy N 50 Years / Male 230120006631NALLA SUDEEP REDDYNo ratings yet
- Technical Dictionary of DancingDocument62 pagesTechnical Dictionary of DancingRory CorbettNo ratings yet
- External Anatomy of The FrogDocument19 pagesExternal Anatomy of The Frogabigail_estrecho83% (6)
- Science 10 Activity Sheet Male and Female Reproductive SystemDocument2 pagesScience 10 Activity Sheet Male and Female Reproductive SystemKarl BadolesNo ratings yet
- What Is Rectum - 3Document9 pagesWhat Is Rectum - 3Ela MarieNo ratings yet
- Biomechanics of Baseball Pitching: Implications For Injury and Performance Glenn Fleisig American Sports Medicine Institute, Birmingham, AL, USADocument5 pagesBiomechanics of Baseball Pitching: Implications For Injury and Performance Glenn Fleisig American Sports Medicine Institute, Birmingham, AL, USAYoh ChenNo ratings yet
- HyperthyroidismDocument12 pagesHyperthyroidismShoppe 'n ShoppersNo ratings yet
- Respiration and Transportation WorksheetDocument4 pagesRespiration and Transportation WorksheetAarjav JainNo ratings yet
- Quick Review - Fossa of RosenmullerDocument4 pagesQuick Review - Fossa of RosenmullerDavis KallanNo ratings yet
- 2008 05 01-Bromley-Head TraumaDocument193 pages2008 05 01-Bromley-Head TraumahanimozaghiNo ratings yet
- Respi Demo Lesson PlanDocument6 pagesRespi Demo Lesson PlanBunny BansNo ratings yet
- Recurrent Laryngeal Nerve Injury During Thyroidectomy - What NextDocument31 pagesRecurrent Laryngeal Nerve Injury During Thyroidectomy - What NextAnisur RahmanNo ratings yet
- Stenosis and Homeopathy - DR Debra KatchenDocument7 pagesStenosis and Homeopathy - DR Debra KatchenSangram007No ratings yet
- Joey: How a Blind Rescue Horse Helped Others Learn to SeeFrom EverandJoey: How a Blind Rescue Horse Helped Others Learn to SeeRating: 5 out of 5 stars5/5 (23)
- Horse Care 101: How to Take Care of a Horse for BeginnersFrom EverandHorse Care 101: How to Take Care of a Horse for BeginnersRating: 4 out of 5 stars4/5 (5)
- The Power of the Herd: A Nonpredatory Approach to Social Intelligence, Leadership, and InnovationFrom EverandThe Power of the Herd: A Nonpredatory Approach to Social Intelligence, Leadership, and InnovationNo ratings yet
- The Faraway Horses: The Adventures and Wisdom of America's Most Renowned HorsemenFrom EverandThe Faraway Horses: The Adventures and Wisdom of America's Most Renowned HorsemenRating: 4.5 out of 5 stars4.5/5 (49)
- Speak Your Horse's Language:: Communicating with the Driving HorseFrom EverandSpeak Your Horse's Language:: Communicating with the Driving HorseNo ratings yet
- How Long Can a Fly Fly?: 175 Answers to Possible and Impossible Questions about AnimalsFrom EverandHow Long Can a Fly Fly?: 175 Answers to Possible and Impossible Questions about AnimalsNo ratings yet
- Traditional Blacksmithing: The Fine Art of Horseshoeing and Wagon MakingFrom EverandTraditional Blacksmithing: The Fine Art of Horseshoeing and Wagon MakingNo ratings yet
- Second-Chance Horses: True Stories of the Horses We Rescue and the Horses Who Rescue UsFrom EverandSecond-Chance Horses: True Stories of the Horses We Rescue and the Horses Who Rescue UsNo ratings yet
- The Everything Horse Book: Buying, riding, and caring for your equine companionFrom EverandThe Everything Horse Book: Buying, riding, and caring for your equine companionRating: 2 out of 5 stars2/5 (1)
- Wild Horses of the Summer Sun: A Memoir of IcelandFrom EverandWild Horses of the Summer Sun: A Memoir of IcelandRating: 3.5 out of 5 stars3.5/5 (4)
- The Winning Horseplayer: An Advanced Approach to Thoroughbred Handicapping and BettingFrom EverandThe Winning Horseplayer: An Advanced Approach to Thoroughbred Handicapping and BettingNo ratings yet
- Building Your Dream Horse: Charles Wilhelm's Ultimate Foundation TrainingFrom EverandBuilding Your Dream Horse: Charles Wilhelm's Ultimate Foundation TrainingRating: 4 out of 5 stars4/5 (4)
- Lead with Your Heart: Lessons from a Life with HorsesFrom EverandLead with Your Heart: Lessons from a Life with HorsesRating: 4 out of 5 stars4/5 (8)
- The USPC Guide to Longeing and Ground TrainingFrom EverandThe USPC Guide to Longeing and Ground TrainingRating: 4.5 out of 5 stars4.5/5 (3)
- Project Solomon: The True Story of a Lonely Horse Who Found a Home--and Became a HeroFrom EverandProject Solomon: The True Story of a Lonely Horse Who Found a Home--and Became a HeroRating: 5 out of 5 stars5/5 (9)
- Stable Relation: A Memoir of One Woman's Spirited Journey Home, by Way of the BarnFrom EverandStable Relation: A Memoir of One Woman's Spirited Journey Home, by Way of the BarnRating: 5 out of 5 stars5/5 (4)
- The Tao Of Horses: Exploring How Horses Guide Us on Our Spiritual PathFrom EverandThe Tao Of Horses: Exploring How Horses Guide Us on Our Spiritual PathRating: 5 out of 5 stars5/5 (1)
- Fitness Evaluation of the HorseFrom EverandFitness Evaluation of the HorseRating: 5 out of 5 stars5/5 (1)
- Hoof Physics: How to Recognize the Signs of Hoof DistortionFrom EverandHoof Physics: How to Recognize the Signs of Hoof DistortionRating: 5 out of 5 stars5/5 (1)
- The Everything Horse Care Book: A Complete Guide to the Well-being of Your HorseFrom EverandThe Everything Horse Care Book: A Complete Guide to the Well-being of Your HorseNo ratings yet
- Horses: 101 Super Fun Facts and Amazing Pictures (Featuring The World's Top 18 Horse Breeds)From EverandHorses: 101 Super Fun Facts and Amazing Pictures (Featuring The World's Top 18 Horse Breeds)Rating: 3.5 out of 5 stars3.5/5 (11)