You might also like
- Small BowelDocument12 pagesSmall BowelURo KkuNo ratings yet
- Anatomy (Length: Duodenum 2.submucosaDocument12 pagesAnatomy (Length: Duodenum 2.submucosaURo KkuNo ratings yet
- Acute AppendicitisDocument5 pagesAcute AppendicitisSHINMEN TAKEZONo ratings yet
- Parietal Cell: Angle of His Angularis IncisuraDocument13 pagesParietal Cell: Angle of His Angularis IncisuraURo Kku100% (1)
- Acute Appendicitis: Incidence SignsDocument4 pagesAcute Appendicitis: Incidence SignsWichien SiriNo ratings yet
- Sx correctable HT renalเRA stenosis, unilat parenchyma dzDocument4 pagesSx correctable HT renalเRA stenosis, unilat parenchyma dzWipaporn ChaengsriNo ratings yet
- Waiting List: Liver Transplantation Renal TransplantDocument2 pagesWaiting List: Liver Transplantation Renal TransplantURo KkuNo ratings yet
- Reflec in SXDocument2 pagesReflec in SXURo KkuNo ratings yet
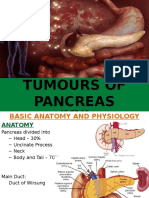
- Tumors of Pancreas DR DilberDocument51 pagesTumors of Pancreas DR Dilberdrdilber100% (1)
- Pgmee Test Series For Neet & Aiims: WWW - Aim4Aiims - In/Pg +91-7529938911Document16 pagesPgmee Test Series For Neet & Aiims: WWW - Aim4Aiims - In/Pg +91-7529938911SHAKEEL1991No ratings yet
- Possible Sign of Superfi V.abnor: 2 Primary FXNDocument7 pagesPossible Sign of Superfi V.abnor: 2 Primary FXNURo KkuNo ratings yet
- Anatomy: - 4 Glands ( 4 Gland 3%) PhysiologicDocument6 pagesAnatomy: - 4 Glands ( 4 Gland 3%) PhysiologicURo KkuNo ratings yet
- Adrenal Cortex: Embryo Cushing SyndDocument7 pagesAdrenal Cortex: Embryo Cushing SyndWichien SiriNo ratings yet
- Sunday, 30 August 2020 1:54 PM: Whitcomb-D-NEJM-2006 PDFDocument2 pagesSunday, 30 August 2020 1:54 PM: Whitcomb-D-NEJM-2006 PDFMichelle De FreitasNo ratings yet
- Test 33: Surgery - Rheumatology/Orthopedics & SportsDocument8 pagesTest 33: Surgery - Rheumatology/Orthopedics & Sportskabal321No ratings yet
- Gas 8Document27 pagesGas 8Triono AssamsulNo ratings yet
- Genitourinary System: Billy Ray A. Marcelo, RNDocument35 pagesGenitourinary System: Billy Ray A. Marcelo, RNDarell M. BookNo ratings yet
- Gastroenterology:: For Questions and Comments Please Go ToDocument4 pagesGastroenterology:: For Questions and Comments Please Go ToSijo SunnyNo ratings yet
- Peritoneal Reflection: AnatomyDocument27 pagesPeritoneal Reflection: AnatomySHINMEN TAKEZONo ratings yet
- Step Up To Medicine Chapter 03Document868 pagesStep Up To Medicine Chapter 03yanks1120No ratings yet
- Severe of Stenosis Unfavor: Carotid A Stenosis Carotid Angioplasty + StentingDocument14 pagesSevere of Stenosis Unfavor: Carotid A Stenosis Carotid Angioplasty + StentingURo Kku100% (1)
- Pancreatitis & Pseudocyst in ChildrenDocument56 pagesPancreatitis & Pseudocyst in ChildrendrkiranmNo ratings yet
- PancreatitisDocument59 pagesPancreatitisAarif RanaNo ratings yet
- Commonly Tested MRCP Part 1 Exam FactsDocument3 pagesCommonly Tested MRCP Part 1 Exam Factssaleema11No ratings yet
- Anaesthesia For Urologic Surgery: (Peer Reviewed) (1987), 15,203-211Document12 pagesAnaesthesia For Urologic Surgery: (Peer Reviewed) (1987), 15,203-211ramzi MohamedNo ratings yet
- Chronic Renal FailureDocument7 pagesChronic Renal FailureSurya Dewi PrimawatiNo ratings yet
- intestinal obstruction 2Document46 pagesintestinal obstruction 2Lawrence WanderiNo ratings yet
- Morning Report Friday, April 5th 2024-2Document8 pagesMorning Report Friday, April 5th 2024-2Tezar AndreanNo ratings yet
- Extrahepatic CholestasisDocument9 pagesExtrahepatic CholestasisMatet MonjeNo ratings yet
- Here Is A List of Commonly Tested Facts in Hte MRCP Part 1 ExamDocument7 pagesHere Is A List of Commonly Tested Facts in Hte MRCP Part 1 Examasallam100% (1)
- Hot GatesDocument38 pagesHot GatesGeorge Mihail ManNo ratings yet
- The Liver: Methods of ExaminationDocument49 pagesThe Liver: Methods of Examinationj.doe.hex_87No ratings yet
- Various Case SeneriosDocument19 pagesVarious Case SeneriosCharu KalraNo ratings yet
- DD - Apendicita AcutaDocument7 pagesDD - Apendicita AcutaAndrea Szasz0% (1)
- Sef de Lucrari DR - Adina PurcareanuDocument24 pagesSef de Lucrari DR - Adina PurcareanuGeorge SimaNo ratings yet
- Portal Hypertension: - DR Sunil Kumar .K.PDocument59 pagesPortal Hypertension: - DR Sunil Kumar .K.PSunil YalodahalliNo ratings yet
- KittenzDocument89 pagesKittenztrina sircarNo ratings yet
- Intussusception CaseDocument19 pagesIntussusception CaseTeena ShamuNo ratings yet
- Carcinoma Pancreas and Periampullary RegionDocument37 pagesCarcinoma Pancreas and Periampullary RegionlallsNo ratings yet
- Feb Recalls 2022 FinalDocument640 pagesFeb Recalls 2022 FinalHafsa Tariq100% (1)
- Curs Abdomen AcutDocument27 pagesCurs Abdomen AcutGabriela AndreeaNo ratings yet
- 155 - B3 Sesi 1 Asisten 2015Document91 pages155 - B3 Sesi 1 Asisten 2015Luthfi AnshoriNo ratings yet
- Cramming Facts for MRCP Part 2 ExamDocument5 pagesCramming Facts for MRCP Part 2 Examxaltra100% (1)
- Carcinoma Pancreas: Risk Factors: (A) Demographic FactorsDocument4 pagesCarcinoma Pancreas: Risk Factors: (A) Demographic FactorsSakthi Annamalai.cNo ratings yet
- Acute Cholecystitis Ppt. DR Dilip S. RajpalDocument42 pagesAcute Cholecystitis Ppt. DR Dilip S. Rajpaldiliprajpal73100% (1)
- Surgery Extra NotesDocument2 pagesSurgery Extra NotesrohalawiNo ratings yet
- 5.-Pancreatita-Cronica ...Document12 pages5.-Pancreatita-Cronica ...Enache MihaiNo ratings yet
- Pancreatic Disease1Document24 pagesPancreatic Disease1Hero StoreNo ratings yet
- Coll. - Tips and Tricks for PLABDocument174 pagesColl. - Tips and Tricks for PLABdrshekarforyouNo ratings yet
- Acute Pancreatitis: Presented By: DAHAL SHIRISHADocument25 pagesAcute Pancreatitis: Presented By: DAHAL SHIRISHASiruNo ratings yet
- Gagal GinjalDocument29 pagesGagal GinjalUniatimelindaNo ratings yet
- Common Complaints of Diseases of The AbdomenDocument37 pagesCommon Complaints of Diseases of The AbdomenNorjetalexis Maningo CabreraNo ratings yet
- Post-void residual volume and bladder scan interpretationDocument7 pagesPost-void residual volume and bladder scan interpretationyanks1120No ratings yet
- Test 41 Qid: 2742: Medicine - Cardiovascular SystemDocument4 pagesTest 41 Qid: 2742: Medicine - Cardiovascular Systemkabal321No ratings yet
- Gastro GuiaDocument17 pagesGastro GuiaLudy Isa IzaNo ratings yet
- 10 StomachDocument10 pages10 StomachApabrita KarmakarNo ratings yet
- CLINICAL HISTORY AND DIFFERENTIAL DIAGNOSIS AT YOUR FINGERTIPSFrom EverandCLINICAL HISTORY AND DIFFERENTIAL DIAGNOSIS AT YOUR FINGERTIPSNo ratings yet
- Fast Facts: Acute and Recurrent Pancreatitis: Using evidence to support treatmentFrom EverandFast Facts: Acute and Recurrent Pancreatitis: Using evidence to support treatmentNo ratings yet
- แบบฝึกหัด Essay 4.1Document1 pageแบบฝึกหัด Essay 4.1URo KkuNo ratings yet
- Abdominal PainDocument76 pagesAbdominal PainURo KkuNo ratings yet
- Case Discussion: Stab Injury L Frank CHFDocument27 pagesCase Discussion: Stab Injury L Frank CHFURo KkuNo ratings yet
- Urologic Imaging For Externist PDFDocument55 pagesUrologic Imaging For Externist PDFURo KkuNo ratings yet
- Perirenal HematomaDocument23 pagesPerirenal HematomaURo KkuNo ratings yet
- Hepatoblastoma ReseachDocument32 pagesHepatoblastoma ReseachURo KkuNo ratings yet
- Malignant Renal TumorDocument17 pagesMalignant Renal TumorURo KkuNo ratings yet
- Ruptured DiverticulitisDocument18 pagesRuptured DiverticulitisURo KkuNo ratings yet
- Histology: GIST Short Note by by S.Wichien (SNG KKU)Document3 pagesHistology: GIST Short Note by by S.Wichien (SNG KKU)URo KkuNo ratings yet
- Mesenteric AdenitisDocument28 pagesMesenteric AdenitisURo KkuNo ratings yet
- LRP PresentationDocument21 pagesLRP PresentationURo KkuNo ratings yet
- Renal Trauma BluntDocument40 pagesRenal Trauma BluntURo KkuNo ratings yet
- GEP NETsDocument3 pagesGEP NETsURo KkuNo ratings yet
- Reflec in SXDocument2 pagesReflec in SXURo KkuNo ratings yet
- แบบฝึกหัด Essay 3Document1 pageแบบฝึกหัด Essay 3URo KkuNo ratings yet
- Reflec in SXDocument2 pagesReflec in SXURo KkuNo ratings yet
- HerniaDocument5 pagesHerniaURo KkuNo ratings yet
- แบบฝึกหัด Essay 3Document1 pageแบบฝึกหัด Essay 3URo KkuNo ratings yet
- UrologyDocument10 pagesUrologyURo KkuNo ratings yet
- Possible Sign of Superfi V.abnor: 2 Primary FXNDocument7 pagesPossible Sign of Superfi V.abnor: 2 Primary FXNURo KkuNo ratings yet
- ColorectalDocument26 pagesColorectalURo KkuNo ratings yet
- LiverDocument13 pagesLiverURo KkuNo ratings yet
- Prophylactic ETT 6yr Fail IV 2: Primary Survey 1.airway 3.circulationDocument17 pagesProphylactic ETT 6yr Fail IV 2: Primary Survey 1.airway 3.circulationURo KkuNo ratings yet
- BreastDocument13 pagesBreastURo KkuNo ratings yet
- Anatomy: - 4 Glands ( 4 Gland 3%) PhysiologicDocument6 pagesAnatomy: - 4 Glands ( 4 Gland 3%) PhysiologicURo KkuNo ratings yet
- SpleenDocument3 pagesSpleenURo KkuNo ratings yet
- Acute PancreatitisDocument36 pagesAcute PancreatitisURo KkuNo ratings yet
- Pass Critical Care Endocrine Frcem ResourcesDocument41 pagesPass Critical Care Endocrine Frcem ResourcesYoussef SaadNo ratings yet
- Unusual Presentation of Pancreatic Insulinoma:a Case ReportDocument5 pagesUnusual Presentation of Pancreatic Insulinoma:a Case ReportIJAR JOURNALNo ratings yet
- Hypoglycemia: Yeditepe University Medical Faculty Department of Endocrinology and MetabolismDocument47 pagesHypoglycemia: Yeditepe University Medical Faculty Department of Endocrinology and MetabolismnawarajNo ratings yet
- Insulin Autoimmune Syndrome: From Diagnosis To Clinical ManagementDocument15 pagesInsulin Autoimmune Syndrome: From Diagnosis To Clinical ManagementClaudia IrimieNo ratings yet
- Insulinoma in A Patient With Type 2 Diabetes: Case Report Nama: Iqbal Putra Amirullah NIM: 030.14.098Document11 pagesInsulinoma in A Patient With Type 2 Diabetes: Case Report Nama: Iqbal Putra Amirullah NIM: 030.14.098desmawitaNo ratings yet
- Insulinoma in an older domestic catDocument3 pagesInsulinoma in an older domestic catRayssa MarleyNo ratings yet
- Pancreatic Solid LeasionsDocument24 pagesPancreatic Solid LeasionsEliza CrăciunNo ratings yet
- Journal of DiabetesDocument6 pagesJournal of DiabetesSartika Rizky HapsariNo ratings yet
- Hypoglycaemia: Presented by Undie, Malipeh-Unim U. House OfficerDocument39 pagesHypoglycaemia: Presented by Undie, Malipeh-Unim U. House OfficerAipee UndieNo ratings yet
- Chemical Pathology 5 - HypoglycaemiaDocument10 pagesChemical Pathology 5 - HypoglycaemiaaNo ratings yet
- Chapter 21 PancreasDocument102 pagesChapter 21 PancreasMACON824No ratings yet
- Gastrinomas Medical or Surgical TreatmentDocument25 pagesGastrinomas Medical or Surgical TreatmentTony Miguel Saba SabaNo ratings yet
- 10 EndocrinologyDocument223 pages10 Endocrinologythisar100% (1)
- Multiple Endocrine NeoplasiaDocument10 pagesMultiple Endocrine NeoplasiacarmenNo ratings yet
- Pankreas DevinDocument12 pagesPankreas DevinDevin ReynandoNo ratings yet
- Hypoglycemia After Gastric Bypass Surgery. Current Concepts and Controversies 2018Document12 pagesHypoglycemia After Gastric Bypass Surgery. Current Concepts and Controversies 2018Rio RomaNo ratings yet
- Canine InsulinomaDocument5 pagesCanine Insulinomasoff4ikaNo ratings yet
- Endocrinology - Review NotesDocument9 pagesEndocrinology - Review NotesRoa Al-SajjanNo ratings yet
- Rodent OncologyDocument24 pagesRodent Oncology黃皓No ratings yet
- EndokrinoDocument78 pagesEndokrinoJulian TaneNo ratings yet
- 10 11648 J Ijde 20200502 12Document4 pages10 11648 J Ijde 20200502 12AdemoluNo ratings yet
- Metabolic Complications of Endocrine Surgery in Companion AnimalsDocument22 pagesMetabolic Complications of Endocrine Surgery in Companion AnimalsEduardo PalaciosNo ratings yet
- 12 Clin Path Exocrine and Endocrine Functions of The PancreasDocument13 pages12 Clin Path Exocrine and Endocrine Functions of The PancreasJolaine ValloNo ratings yet
- Cystic LesionsDocument101 pagesCystic LesionsKartik GuptaNo ratings yet
- Causes of Hypoglycemia in Infants and ChildrenDocument18 pagesCauses of Hypoglycemia in Infants and ChildrenhelviNo ratings yet
- Surgery 3 - Answers v1 (Wide)Document57 pagesSurgery 3 - Answers v1 (Wide)Humzala BashamNo ratings yet
- Singkatan MnemonicsDocument4 pagesSingkatan MnemonicsguterizalNo ratings yet
- HypoglycemiaDocument113 pagesHypoglycemiamadelleinetNo ratings yet
- 7325-300 C-Peptide & Insulin AccuBind VAST ELISA Rev 6Document2 pages7325-300 C-Peptide & Insulin AccuBind VAST ELISA Rev 6Luisa MaríaNo ratings yet
- Hypoglycemia UMYDocument60 pagesHypoglycemia UMYTommy AkromaNo ratings yet