You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Topic English EssayDocument8 pagesTopic English Essayd3gpmvqw100% (2)
- Func - Samplebooklet - Libro Gratis de Muestra Pivot PointDocument81 pagesFunc - Samplebooklet - Libro Gratis de Muestra Pivot PointRaquel100% (1)
- Hepatita B ProiectDocument3 pagesHepatita B ProiectaleecssandraaNo ratings yet
- HBIDocument16 pagesHBITanmay GhoshNo ratings yet
- Occupational Hazards in Dentistry: Acta Scientific DENTAL SCIENCES (ISSN: 2581-4893)Document7 pagesOccupational Hazards in Dentistry: Acta Scientific DENTAL SCIENCES (ISSN: 2581-4893)nioh envisNo ratings yet
- Global Hepatitis Report 2024 1-10Document10 pagesGlobal Hepatitis Report 2024 1-10Ştefaniuc IulianNo ratings yet
- Paeds McqsDocument4 pagesPaeds McqsSidra JavedNo ratings yet
- Hepatitis B (HBV) : 2-Months RegimenDocument20 pagesHepatitis B (HBV) : 2-Months Regimenulovemusicsodoi7799No ratings yet
- MCN II NewbornDocument14 pagesMCN II NewbornJharaNo ratings yet
- Knowledge of Hepatitis B Virus Infection Among Traders: Original ArticleDocument6 pagesKnowledge of Hepatitis B Virus Infection Among Traders: Original ArticleMark Philipp AbanNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaRoman DiazNo ratings yet
- Hepatitis Viral AkutDocument50 pagesHepatitis Viral AkutJonovSelfNo ratings yet
- Plant Molecular Farming For Recombinant Therapeutic ProteinsDocument61 pagesPlant Molecular Farming For Recombinant Therapeutic Proteinsnitin_star2010No ratings yet
- Cipla Product ListDocument33 pagesCipla Product ListSumit Singhania100% (2)
- HCV Riba ChironDocument25 pagesHCV Riba ChironPrasanth GovindanNo ratings yet
- 10 3 2 Ijmr PDFDocument4 pages10 3 2 Ijmr PDFSindhu ShreeNo ratings yet
- Work Policy On Hepatitis BDocument3 pagesWork Policy On Hepatitis BPauline Mae AranetaNo ratings yet
- Big Group A1 General Task 1 Nursing AssessmentDocument15 pagesBig Group A1 General Task 1 Nursing AssessmentCAUSIN, Lance Matthew,No ratings yet
- Hepatitis A & B Power PointDocument15 pagesHepatitis A & B Power PointHerlina Marshal100% (1)
- Hepatitis BDocument5 pagesHepatitis BAmple CasaclangNo ratings yet
- Virology MCQ 1Document21 pagesVirology MCQ 1Robert Edwards100% (9)
- Home-Made HBsAgDocument1 pageHome-Made HBsAgsomchaisNo ratings yet
- Hepatitis D Virus (HDV) : PathogenesisDocument30 pagesHepatitis D Virus (HDV) : PathogenesisJc GaldosNo ratings yet
- Medical Funnotes VolumeDocument108 pagesMedical Funnotes VolumeChinNo ratings yet
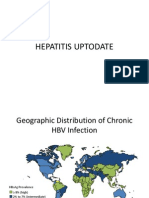
- Hepatitis UptodateDocument15 pagesHepatitis UptodateRicardo ChavezNo ratings yet
- Plasmapheresis For AutoimmunityDocument14 pagesPlasmapheresis For AutoimmunityEliDavidNo ratings yet
- Hepatitis BDocument61 pagesHepatitis BMichael AmandyNo ratings yet
- Needle Stick InjuriesDocument24 pagesNeedle Stick InjuriesSarthak LaboratoryNo ratings yet
- Hepa BDocument2 pagesHepa BKhristine Joy Constantino AntiguaNo ratings yet
- Take Away 2 - Airbus Hazard Prevention Handbook (Distribution Copy)Document41 pagesTake Away 2 - Airbus Hazard Prevention Handbook (Distribution Copy)UbernatorNo ratings yet