You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
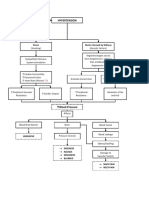
- Hypertension Concept MapDocument1 pageHypertension Concept Mapjyd parreñoNo ratings yet
- Approach To AscitesDocument88 pagesApproach To AscitesKartheek VarmaNo ratings yet
- M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument23 pagesM.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Pharm Fall Cardiovascular Pharmacology Study Guide-106Document47 pagesPharm Fall Cardiovascular Pharmacology Study Guide-106sean liyanageNo ratings yet
- Physiology RAASDocument3 pagesPhysiology RAASAulia Mahya FaradisaNo ratings yet
- Urinary SystemDocument95 pagesUrinary SystemCloud D. LuffyNo ratings yet
- Chapter 27 GuytonDocument6 pagesChapter 27 GuytonGabriella ChafrinaNo ratings yet
- Hypertension: Department of Internal MedicineDocument58 pagesHypertension: Department of Internal MedicineLouije MombzNo ratings yet
- Seminar: Kamyar Kalantar-Zadeh, Tazeen H Jafar, Dorothea Nitsch, Brendon L Neuen, Vlado PerkovicDocument17 pagesSeminar: Kamyar Kalantar-Zadeh, Tazeen H Jafar, Dorothea Nitsch, Brendon L Neuen, Vlado PerkovicDanny Bolaño MartinezNo ratings yet
- Case Study CHF Final Output Group 2Document83 pagesCase Study CHF Final Output Group 2SHEILA MAE SACLOTNo ratings yet
- CVS Lect 6 Blood Pressure, PathophysiologyDocument13 pagesCVS Lect 6 Blood Pressure, PathophysiologySherwan R Shal100% (5)
- ACE Inhibitors Vs ARBsDocument3 pagesACE Inhibitors Vs ARBsKo Phyo WaiNo ratings yet
- ACE InhibitorsDocument26 pagesACE Inhibitorsali mohammedNo ratings yet
- SGLT2 Inhibitors and Mechanisms of Cardiovascular Benefit: A State-Of-The-Art ReviewDocument10 pagesSGLT2 Inhibitors and Mechanisms of Cardiovascular Benefit: A State-Of-The-Art ReviewLucian SiriteanuNo ratings yet
- Excretory Products and Their Elimination - UnacademyDocument79 pagesExcretory Products and Their Elimination - UnacademyDEVENDRA kumar SahuNo ratings yet
- REGULATION OF FLUID AND ELECTROLYTE BALANCEDocument18 pagesREGULATION OF FLUID AND ELECTROLYTE BALANCEKim RamosNo ratings yet
- NCM 106 - Week 2 (Cardiovascular P1) (Midterm)Document7 pagesNCM 106 - Week 2 (Cardiovascular P1) (Midterm)MARIA KAWILANNo ratings yet
- 7-Moto Renal - MCQsDocument62 pages7-Moto Renal - MCQspvs5155No ratings yet
- FSG332 Cardiovascular Pathophysiology 3 - 2Document39 pagesFSG332 Cardiovascular Pathophysiology 3 - 2Huzaifa KhanNo ratings yet
- CA0002OCDocument27 pagesCA0002OCYourChemistryTeacherNo ratings yet
- Combizar Drug StudyDocument6 pagesCombizar Drug StudymrnmrsllNo ratings yet
- Heart Failure Guide for NursesDocument54 pagesHeart Failure Guide for NursesKacelyn QuibanNo ratings yet
- Chapter 19Document6 pagesChapter 19Teehee JonesNo ratings yet
- NCP TbiDocument4 pagesNCP TbiWyen CabatbatNo ratings yet
- Electrolyte Abnormalities GuideDocument15 pagesElectrolyte Abnormalities GuideCecilia GrayebNo ratings yet
- Tmp1a96 TMPDocument80 pagesTmp1a96 TMPFrontiersNo ratings yet
- Philip Kalra PDFDocument38 pagesPhilip Kalra PDFDennis JakeNo ratings yet
- 4 5787572421108171420 PDFDocument62 pages4 5787572421108171420 PDFnanda1al1humairahNo ratings yet
- Cardiovascular NotesDocument23 pagesCardiovascular NotesEmily DongNo ratings yet
- Nutrition Therapy and Pathophysiology 3rd Edition Nelms Test BankDocument16 pagesNutrition Therapy and Pathophysiology 3rd Edition Nelms Test Bankrorybridgetewe100% (22)