You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Biopsychosocial AssessmentDocument8 pagesBiopsychosocial AssessmentAnn OgoloNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Ambulatory Surgical CareDocument265 pagesAmbulatory Surgical CareThamizhanban R100% (2)
- Quick Selection of Chinese Herbal Formulas Based On Clinical ConditionsDocument0 pagesQuick Selection of Chinese Herbal Formulas Based On Clinical Conditionsharbor100% (1)
- The Principle of Cataract Surgery: Andari Putri WardhaniDocument16 pagesThe Principle of Cataract Surgery: Andari Putri WardhaniAndari Putri WardhaniNo ratings yet
- Anesthesiology PDFDocument40 pagesAnesthesiology PDFBiswajyoti SahuNo ratings yet
- Patient Satisfaction SurveyDocument3 pagesPatient Satisfaction SurveyGlady Jane TevesNo ratings yet
- The Code of Ethics For NursesDocument8 pagesThe Code of Ethics For NursesZulkifli PomalangoNo ratings yet
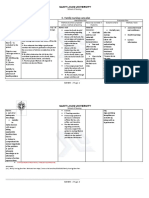
- C. Family Nursing Care Plan: Saint Louis UniversityDocument2 pagesC. Family Nursing Care Plan: Saint Louis UniversityLEONELLGABRIEL RAGUINDIN0% (1)
- Bag TechniqueDocument23 pagesBag TechniqueMamta Rajput83% (12)
- Company Profile Complete VersionDocument13 pagesCompany Profile Complete VersionJanna FabiaNo ratings yet
- Dialog Bahasa Inggris5Document3 pagesDialog Bahasa Inggris5MilNo ratings yet
- Meedical History FormDocument3 pagesMeedical History FormSonja OsmanovićNo ratings yet
- SURESH Testing ProfileDocument3 pagesSURESH Testing Profilefreecharge momNo ratings yet
- Parathyroid ScintigraphyDocument6 pagesParathyroid Scintigraphyahmedmaksoud2036No ratings yet
- Changes in Brain Function (Quantitative EEG Cordance) During Placebo Lead-In and Treatment Outcomes in Clinical Trials For Major DepressionDocument7 pagesChanges in Brain Function (Quantitative EEG Cordance) During Placebo Lead-In and Treatment Outcomes in Clinical Trials For Major DepressiondebdotnetNo ratings yet
- Dental AssistantDocument3 pagesDental Assistantapi-78766098No ratings yet
- Drug Study of FractureDocument3 pagesDrug Study of FractureMarijune Caban ViloriaNo ratings yet
- NCP of Chronic Renal FailureDocument2 pagesNCP of Chronic Renal FailureElusiveNo ratings yet
- CVDocument2 pagesCVapi-326166436No ratings yet
- ADR News Dec2008 Vol10 No3Document8 pagesADR News Dec2008 Vol10 No3William ChandraNo ratings yet
- Post Graduate Academic Report Vion FinalDocument18 pagesPost Graduate Academic Report Vion FinalVishali RayapudiNo ratings yet
- Effects of Activator and High Pull Headgear Combination Therapy PDFDocument9 pagesEffects of Activator and High Pull Headgear Combination Therapy PDFDilesh PradhanNo ratings yet
- Lax Child Cling D LineDocument1 pageLax Child Cling D LineemjaeNo ratings yet
- Anxiety Disorders in ChildrenDocument3 pagesAnxiety Disorders in ChildrenooiseowwweiNo ratings yet
- Mergency Medicine, Second Edition: 60 Acid-Base DisordersDocument21 pagesMergency Medicine, Second Edition: 60 Acid-Base DisordersLukman NurfauziNo ratings yet
- Zolendronat NEJMDocument11 pagesZolendronat NEJMnoveldycb89No ratings yet
- SAAOL Heart Centre CaseDocument9 pagesSAAOL Heart Centre CaseMunem ChowdhuryNo ratings yet
- The Pathophysiology of Alzheimer'S Disease and Directions in TreatmentDocument15 pagesThe Pathophysiology of Alzheimer'S Disease and Directions in TreatmentEnerolisa ParedesNo ratings yet
- Maxillary Major ConnectorsDocument20 pagesMaxillary Major ConnectorsRohan GroverNo ratings yet
- Jurnal Code Blue PDFDocument4 pagesJurnal Code Blue PDFAfi Adi KiranaNo ratings yet