You might also like
- Surgery IIExam 1 REVIEWDocument6 pagesSurgery IIExam 1 REVIEWEddie MillsNo ratings yet
- Medial Column Flatfoot SurgeryDocument2 pagesMedial Column Flatfoot SurgeryEddie MillsNo ratings yet
- Calcaneal Varus, Forfootvarus, PF1 Stray, EquinusDocument2 pagesCalcaneal Varus, Forfootvarus, PF1 Stray, EquinusEddie MillsNo ratings yet
- Surgery 1 - 1st ray-MTPJ (1-25-08)Document3 pagesSurgery 1 - 1st ray-MTPJ (1-25-08)Eddie MillsNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Olympic Sports Evolution Over TimeDocument6 pagesOlympic Sports Evolution Over TimeJr FloresNo ratings yet
- Halo Fleet Battles FAQ Errata and Clarifications PDFDocument4 pagesHalo Fleet Battles FAQ Errata and Clarifications PDFSam VeeversNo ratings yet
- Physical Fitness: Group 3 Members: Ali, Mycah Therese Hibuton, Jessa Sanguila, Aminah Canque, Nicole Ombawa, OmayyahDocument13 pagesPhysical Fitness: Group 3 Members: Ali, Mycah Therese Hibuton, Jessa Sanguila, Aminah Canque, Nicole Ombawa, OmayyahjessaNo ratings yet
- Land Cruiser V8 Towbar Wiring Kit InstallDocument31 pagesLand Cruiser V8 Towbar Wiring Kit InstallVladimir TereshchenkoNo ratings yet
- Export SapDocument10 pagesExport SapLuisNo ratings yet
- Dominate Sports BettingDocument38 pagesDominate Sports Bettingmaximaurelian50% (2)
- Pipeline Design and ConstructionDocument47 pagesPipeline Design and ConstructionSaber Abdel Moreid100% (5)
- Nutrition 3Document2 pagesNutrition 3azszahNo ratings yet
- 1616 ToDocument4 pages1616 TohamzajmorshedNo ratings yet
- NP + TV (E12) (Key Lien)Document41 pagesNP + TV (E12) (Key Lien)Linh HoàngNo ratings yet
- Correlated Subqueries: Mona KhalilDocument40 pagesCorrelated Subqueries: Mona Khalilanubhav582No ratings yet
- 01 Viktor Korchnoi - WikipediaDocument8 pages01 Viktor Korchnoi - WikipediaAThaddeusAntonioNo ratings yet
- RFP 28 Day Pilates Challenge 2024Document1 pageRFP 28 Day Pilates Challenge 2024Carol ChanNo ratings yet
- Pinoy TambayanDocument33 pagesPinoy TambayanPinoy TvNo ratings yet
- Understanding Muscle PhysiologyDocument88 pagesUnderstanding Muscle Physiologyandre andreNo ratings yet
- Despiece Ensobradora Pitney Bowes Di380 PDFDocument132 pagesDespiece Ensobradora Pitney Bowes Di380 PDFLuis GuerreroNo ratings yet
- Resident Evil 4 - Wii Edition (USA) (En, De)Document5 pagesResident Evil 4 - Wii Edition (USA) (En, De)Valentino RaynaldiNo ratings yet
- King of Ears Torture DemonDocument1 pageKing of Ears Torture DemonMatt AmorosoNo ratings yet
- Auto Trans Diagnosis - Aw03-72Le Article TextDocument15 pagesAuto Trans Diagnosis - Aw03-72Le Article TextLeonardo SilvaNo ratings yet
- Parts List of Engine Assy of FMX 440 (PC-24) - TP-836Document1 pageParts List of Engine Assy of FMX 440 (PC-24) - TP-836Cws0% (1)
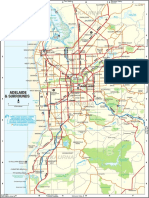
- Map Adelaide SuburbsDocument1 pageMap Adelaide SuburbsJitender YadavNo ratings yet
- DC09 072A. 289-358 KW (329-405 kVA) : Fuel OptimizedDocument2 pagesDC09 072A. 289-358 KW (329-405 kVA) : Fuel OptimizedJulio SullaymeNo ratings yet
- IOCL World Cup Contest Winner Match 34 35 36 37Document59 pagesIOCL World Cup Contest Winner Match 34 35 36 37JaminiNo ratings yet
- P.E. 7 - Q1 - Module1bDocument17 pagesP.E. 7 - Q1 - Module1breymilyn zuluetaNo ratings yet
- Cyl LinerDocument3 pagesCyl LinerAkang OntohodNo ratings yet
- Pro StarDocument263 pagesPro StarLuis EduardoNo ratings yet
- The Lost Battalion EssayDocument2 pagesThe Lost Battalion Essayapi-336625608100% (1)
- Air StarterDocument6 pagesAir StarterParvizNo ratings yet
- SBOKC2023 Bulletin 3.0Document22 pagesSBOKC2023 Bulletin 3.0Andi YusufNo ratings yet
- Tenses Class 11Document4 pagesTenses Class 11harshitaNo ratings yet