You might also like
- 1.1 Million: Philippines: Typhoon Haiyan - Humanitarian SnapshotDocument1 page1.1 Million: Philippines: Typhoon Haiyan - Humanitarian Snapshotmarkleongoldber3215No ratings yet
- Initial Management of Contaminated PatientsDocument21 pagesInitial Management of Contaminated Patientsmarkleongoldber3215No ratings yet
- AVAC AIDS Tipping PointDocument1 pageAVAC AIDS Tipping PointmurphmanNo ratings yet
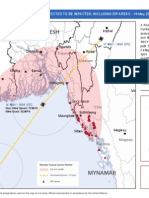
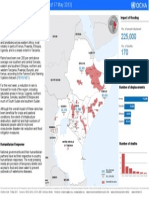
- Cyclone Ma HasenDocument1 pageCyclone Ma Hasenmarkleongoldber3215No ratings yet
- Eastern Africa Floods Update 17 May 2013Document1 pageEastern Africa Floods Update 17 May 2013markleongoldber3215No ratings yet
- ClimasphereDocument1 pageClimaspheremarkleongoldber3215No ratings yet
- Syria Numbers and Locations of Refugees and IDPsDocument1 pageSyria Numbers and Locations of Refugees and IDPsmarkleongoldber3215No ratings yet
- Syria DisplacementlRefugees 2013apr05 HIU U770Document1 pageSyria DisplacementlRefugees 2013apr05 HIU U770markleongoldber3215No ratings yet
- Ocha FundingDocument2 pagesOcha Fundingmarkleongoldber3215No ratings yet
- Hurricane - Sandy 26 October 2012petitDocument1 pageHurricane - Sandy 26 October 2012petitmarkleongoldber3215No ratings yet
- Cyclone Ma HasenDocument1 pageCyclone Ma Hasenmarkleongoldber3215No ratings yet
- Worldwide HumanitarianAidWorkers 2012aug15 HIU U618Document1 pageWorldwide HumanitarianAidWorkers 2012aug15 HIU U618markleongoldber3215No ratings yet
- RMMS September MapDocument1 pageRMMS September Mapmarkleongoldber3215No ratings yet
- TB in South African MinesDocument2 pagesTB in South African Minesmarkleongoldber3215No ratings yet
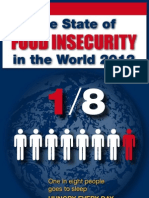
- FAO Infographic SOFI 2012 enDocument1 pageFAO Infographic SOFI 2012 enmarkleongoldber3215No ratings yet
- Map of The DayDocument1 pageMap of The Daymarkleongoldber3215No ratings yet
- Unhcr Pop of ConcernDocument2 pagesUnhcr Pop of Concernmarkleongoldber3215No ratings yet
- Lebanon RefugeesDocument1 pageLebanon Refugeesmarkleongoldber3215No ratings yet
- Speaker Series InvitationDocument1 pageSpeaker Series Invitationmarkleongoldber3215No ratings yet
- Rotary Info Graphic FINALDocument2 pagesRotary Info Graphic FINALmarkleongoldber3215No ratings yet
- Saving at BirthDocument1 pageSaving at Birthmarkleongoldber3215No ratings yet
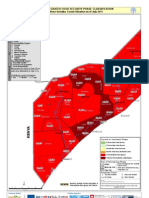
- Famine MapDocument1 pageFamine Mapmarkleongoldber3215No ratings yet
- Fall 2011 UN Polling MemoDocument9 pagesFall 2011 UN Polling Memomarkleongoldber3215No ratings yet
- UN Polling Data1Document8 pagesUN Polling Data1markleongoldber3215No ratings yet
- Map 1293Document2 pagesMap 1293markleongoldber3215No ratings yet
- PakfloodsDocument1 pagePakfloodsmarkleongoldber3215No ratings yet
- MogadishuDocument1 pageMogadishumarkleongoldber3215No ratings yet
- Somalia MapDocument2 pagesSomalia Mapmarkleongoldber3215No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 8.review Meenu Mary PaulDocument10 pages8.review Meenu Mary PaulDilmohit SinghNo ratings yet
- Hygiene Sanitasi Organ Genetalia WanitaDocument25 pagesHygiene Sanitasi Organ Genetalia WanitaYunita Tri JayatiNo ratings yet
- History of the stethoscopeDocument2 pagesHistory of the stethoscopepswaminathan100% (1)
- AutismDocument2 pagesAutismGlenn GraystonNo ratings yet
- Kolkata Medical Facilities ListDocument10 pagesKolkata Medical Facilities ListMrinal ChakrabortyNo ratings yet
- Dental FluorosisDocument8 pagesDental Fluorosiskuantumonline100% (1)
- Cebu Declaration List of ParticipantsDocument6 pagesCebu Declaration List of ParticipantspuspaNo ratings yet
- Injuries in YogaDocument30 pagesInjuries in YogaKalpak Shah100% (1)
- Dental Liaison Committee in The EUDocument545 pagesDental Liaison Committee in The EUirinalully100% (1)
- Commercial Index - SV - CarlislecDocument308 pagesCommercial Index - SV - CarlislecRobert RangstanNo ratings yet
- Hospital Interior Designing Services PDFDocument6 pagesHospital Interior Designing Services PDFreddi.demullu007No ratings yet
- Girls Who Masturbate in Early Infancy: Diagnostics, Natural Course and A Long-Term Follow-UpDocument5 pagesGirls Who Masturbate in Early Infancy: Diagnostics, Natural Course and A Long-Term Follow-UpNurdin Aji IskandarNo ratings yet
- History Taking and Clinical ExaminationDocument34 pagesHistory Taking and Clinical Examinationrinaldi100% (1)
- Sports DentistryDocument11 pagesSports DentistryMaqbul AlamNo ratings yet
- Kinesiotaping Research AbstractsDocument43 pagesKinesiotaping Research AbstractsWladimir HirthNo ratings yet
- Definition of A Pediatrician: Pediatrics April 2015Document5 pagesDefinition of A Pediatrician: Pediatrics April 2015Fiqri VengeanceHanerNo ratings yet
- Elbow ExaminationelDocument3 pagesElbow ExaminationelAboud AbbassiNo ratings yet
- Fixation of The Distal Tibiofibular Bone-Bridge in Transtibial Amputation PDFDocument4 pagesFixation of The Distal Tibiofibular Bone-Bridge in Transtibial Amputation PDFThomas BowersNo ratings yet
- Scholars For Medicine EssayDocument3 pagesScholars For Medicine EssaySiddharth ShethNo ratings yet
- PERINATAL PATIENT SAFETY: Management of Oxytocin For Labor Induction and Augmentation MCN, The American Journal of Maternal/Child NursingDocument2 pagesPERINATAL PATIENT SAFETY: Management of Oxytocin For Labor Induction and Augmentation MCN, The American Journal of Maternal/Child NursingNishaThakuriNo ratings yet
- Meisinger KatalogDocument107 pagesMeisinger KatalogRabshaqaNo ratings yet
- WFA Competency LevelsDocument5 pagesWFA Competency LevelsTroy Lyons DunowNo ratings yet
- Manual de Entrenamiento Ventilador de Anestesia Blease 8500Document69 pagesManual de Entrenamiento Ventilador de Anestesia Blease 8500Roberto Ramírez80% (5)
- General AnaesthesiaDocument53 pagesGeneral Anaesthesiapeter singal100% (2)
- CSH Perspectives Rev - Apolipoprotein E and Apolipoprotein E Receptors - Normal Biology and Roles in ADDocument23 pagesCSH Perspectives Rev - Apolipoprotein E and Apolipoprotein E Receptors - Normal Biology and Roles in ADGeneziz DiazNo ratings yet
- Figo Staging Systems 2009 Uterine SarcomaDocument1 pageFigo Staging Systems 2009 Uterine SarcomalokdonlubNo ratings yet
- Daftar Pustaka HEGDocument2 pagesDaftar Pustaka HEGJennifer BrockNo ratings yet
- Camp Rap-A-Hope - 2013 Annual ReportDocument20 pagesCamp Rap-A-Hope - 2013 Annual ReportWest SandersNo ratings yet
- Talar Fracture Rehab PhasesDocument4 pagesTalar Fracture Rehab PhasesAlexandra NadinneNo ratings yet
- CGHS-Approved Hospitals ListDocument9 pagesCGHS-Approved Hospitals Listgarg_mahak3199No ratings yet