You might also like
- Case Study RPH TanawanDocument20 pagesCase Study RPH TanawanKarlo BartolomeNo ratings yet
- Pamantasan NG Cabuyao College of Health Allied Sciences College of NursingDocument43 pagesPamantasan NG Cabuyao College of Health Allied Sciences College of NursingSofea MustaffaNo ratings yet
- Pneumonia Case PresentationDocument102 pagesPneumonia Case PresentationRegineCuasSulibNo ratings yet
- Case Presentation: Patient Chart - Mary JohnsonDocument12 pagesCase Presentation: Patient Chart - Mary Johnsonivoneeh_16100% (1)
- Pediatric CAP & Dengue Case PresentationDocument92 pagesPediatric CAP & Dengue Case PresentationSuzette Rae TateNo ratings yet
- Patient History for J.M.CDocument13 pagesPatient History for J.M.Cbonziebuddy100% (1)
- Nursing Care Plan for Pediatric Community Acquired PneumoniaDocument35 pagesNursing Care Plan for Pediatric Community Acquired PneumoniaJose Bryan NacillaNo ratings yet
- Pulmonary TuberculosisDocument46 pagesPulmonary Tuberculosisroseann_808100% (1)
- Acute Bronchiolitis TreatmentDocument36 pagesAcute Bronchiolitis TreatmentPyka Izzaty100% (1)
- TB Case StudyDocument2 pagesTB Case StudyReisabelle LabianoNo ratings yet
- Thyroid Papillary Carcinoma CaseDocument6 pagesThyroid Papillary Carcinoma CaseRandy F BabaoNo ratings yet
- Manila colleges nursing process on Dengue Hemorrhagic FeverDocument14 pagesManila colleges nursing process on Dengue Hemorrhagic FeverShell BalangueNo ratings yet
- Pneumonia PresentationDocument20 pagesPneumonia PresentationsetanpikulanNo ratings yet
- Sudden Infant Death SyndromeDocument5 pagesSudden Infant Death SyndromeJanelle Gift SenarloNo ratings yet
- Anatomy and Phsyiology of MeningococcemiaDocument2 pagesAnatomy and Phsyiology of MeningococcemiaKevin Comahig100% (1)
- Typhoid Fever: Pathophysiology, Signs, Symptoms and Nursing CareDocument13 pagesTyphoid Fever: Pathophysiology, Signs, Symptoms and Nursing CareCassey CuregNo ratings yet
- Teaching Case Presentation 2Document20 pagesTeaching Case Presentation 2api-347034408No ratings yet
- CPM 10th Ed Community Acquired PneumoniaDocument23 pagesCPM 10th Ed Community Acquired PneumoniaJan Mikhail FrascoNo ratings yet
- NCP Poststreptococcal GlomerulonephritisDocument12 pagesNCP Poststreptococcal GlomerulonephritisScarlet ScarletNo ratings yet
- Hepatocellular Carcinoma: Hepatocellular Carcinoma (HCC, Also Called Malignant Hepatoma) Is The MostDocument10 pagesHepatocellular Carcinoma: Hepatocellular Carcinoma (HCC, Also Called Malignant Hepatoma) Is The MostNurul An NisaNo ratings yet
- Dengue Hemorrhagic FeverDocument9 pagesDengue Hemorrhagic FevermarianegvNo ratings yet
- COPD End-Stage Symptoms Treatments OutlookDocument15 pagesCOPD End-Stage Symptoms Treatments OutlookAlexandra T ManzanoNo ratings yet
- Hepatitis overview and nursing careDocument18 pagesHepatitis overview and nursing careAnne B. BuenvenidaNo ratings yet
- Case StudyDocument41 pagesCase StudyAubrey Ann FolloscoNo ratings yet
- HPV Virus Causes Recurrent Respiratory Papillomatosis in BoyDocument21 pagesHPV Virus Causes Recurrent Respiratory Papillomatosis in BoyDaffa IbnurasyNo ratings yet
- IM AdconDocument28 pagesIM AdconCla SantosNo ratings yet
- Bacterial and Viral MeningitisDocument12 pagesBacterial and Viral Meningitisapi-3704562No ratings yet
- Case Study DengueDocument11 pagesCase Study DengueCarl Julienne MasangcayNo ratings yet
- Acute Pneumonia: Richard T. Ellison III and Gerald R. DonowitzDocument30 pagesAcute Pneumonia: Richard T. Ellison III and Gerald R. DonowitzNilay ChatterjeeNo ratings yet
- Gallstone Case StudyDocument19 pagesGallstone Case StudyMoNa JbaReenNo ratings yet
- ACute Pylonephris Case PresentationDocument6 pagesACute Pylonephris Case PresentationbantilanNo ratings yet
- Typhoid FeverDocument38 pagesTyphoid FeverRonelenePurisimaNo ratings yet
- Coughs and Colds Nurse Management of Upper Respiratory Tract InfectionDocument3 pagesCoughs and Colds Nurse Management of Upper Respiratory Tract InfectionMichael Anthony ErmitaNo ratings yet
- Febrile SeizureDocument6 pagesFebrile SeizurepipimseptianaNo ratings yet
- MDRTB Case StudyDocument35 pagesMDRTB Case StudyFejlean Angelica AntineoNo ratings yet
- THROMBOPHLEBITISDocument50 pagesTHROMBOPHLEBITISmers puno100% (3)
- Papillary Thyroid Ca: Group. 1 B Grand CaseDocument16 pagesPapillary Thyroid Ca: Group. 1 B Grand CaseAdora Dela CruzNo ratings yet
- Case Study PneumoniaDocument6 pagesCase Study PneumoniaBrian CornelNo ratings yet
- Case 3 DengueDocument19 pagesCase 3 DengueJane LaquihonNo ratings yet
- Pulmonary Tuberculosis (PTB)Document6 pagesPulmonary Tuberculosis (PTB)carls burg a. resurreccion100% (2)
- NCP DHFDocument3 pagesNCP DHFjsdc_14No ratings yet
- Pa Tho PhysiologyDocument3 pagesPa Tho Physiologyaprilkow07No ratings yet
- Dengue Fever: Causes, Symptoms and PreventionDocument7 pagesDengue Fever: Causes, Symptoms and PreventionAmber Hope PonsicaNo ratings yet
- Seizure DisorderDocument4 pagesSeizure DisorderJohanna ChavezNo ratings yet
- Acute Lobar PneumoniaDocument13 pagesAcute Lobar PneumoniaICNo ratings yet
- NSTEMIDocument33 pagesNSTEMIwaazalimahwahidNo ratings yet
- PCAP-C Endorsement NotesDocument2 pagesPCAP-C Endorsement NotesLorraine GambitoNo ratings yet
- Ulcerative ColitisDocument18 pagesUlcerative ColitisHoussein EL HajjNo ratings yet
- BFCDocument8 pagesBFCIrene GunongNo ratings yet
- HTN Urgency Case StudyDocument4 pagesHTN Urgency Case StudyJavin TNo ratings yet
- Acute Respiratory Distress SyndromDocument38 pagesAcute Respiratory Distress SyndrompatriaindraNo ratings yet
- USC Case 04 - SinusitisDocument9 pagesUSC Case 04 - SinusitisDisti Damelia SebayangNo ratings yet
- Dehydration Symptoms and Treatment PlansDocument2 pagesDehydration Symptoms and Treatment PlansJennyu YuNo ratings yet
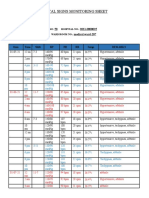
- Vital Signs Monitoring SheetDocument2 pagesVital Signs Monitoring SheetRenea Joy ArruejoNo ratings yet
- A Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutFrom EverandA Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutRating: 5 out of 5 stars5/5 (1)
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Health Is Definitely A Significant Element of Life OptimizationDocument7 pagesHealth Is Definitely A Significant Element of Life Optimizationana_monteron8096No ratings yet
- Liceo de Cagayan University College of Nursing Ncm501202 Related LearningDocument22 pagesLiceo de Cagayan University College of Nursing Ncm501202 Related LearningivaniansNo ratings yet
- Acute Bronchitis Care Study 202Document25 pagesAcute Bronchitis Care Study 202Kara Kathrina FuentesNo ratings yet
- House Hold Profile and Vaccination StatusDocument2 pagesHouse Hold Profile and Vaccination StatusKylie GolindangNo ratings yet
- House Hold Profile and Vaccination StatusDocument2 pagesHouse Hold Profile and Vaccination StatusKylie GolindangNo ratings yet
- List of 0 - 11 MonthsDocument2 pagesList of 0 - 11 MonthsKylie GolindangNo ratings yet
- Creation God's Plan of The AgesDocument101 pagesCreation God's Plan of The AgesLV GraphicsNo ratings yet
- Cot 3Document4 pagesCot 3Kylie GolindangNo ratings yet
- CV - KBGDocument6 pagesCV - KBGKylie GolindangNo ratings yet
- THE-CASE-OFDocument8 pagesTHE-CASE-OFKylie GolindangNo ratings yet
- How to Receive Eternal Life Through Faith in Jesus ChristDocument16 pagesHow to Receive Eternal Life Through Faith in Jesus ChristKylie GolindangNo ratings yet
- TheoriesDocument2 pagesTheoriesKylie GolindangNo ratings yet
- Attendance Logbook2Document1 pageAttendance Logbook2Kylie GolindangNo ratings yet
- LaawDocument1 pageLaawKylie GolindangNo ratings yet
- Drug AddictionDocument12 pagesDrug AddictionKylie GolindangNo ratings yet
- Share Your Point of View KBGDocument2 pagesShare Your Point of View KBGKylie GolindangNo ratings yet
- Cot 1Document4 pagesCot 1Kylie GolindangNo ratings yet
- Cot 4Document5 pagesCot 4Kylie GolindangNo ratings yet
- Reading Passage 4Document11 pagesReading Passage 4Kylie GolindangNo ratings yet
- Cot 2Document4 pagesCot 2Kylie GolindangNo ratings yet
- GOLINDANGDocument3 pagesGOLINDANGKylie GolindangNo ratings yet
- How I was floored by a tick reveals Lyme disease diagnosis journeyDocument12 pagesHow I was floored by a tick reveals Lyme disease diagnosis journeyKylie GolindangNo ratings yet
- Budget Stages - Kyle - GolindangDocument17 pagesBudget Stages - Kyle - GolindangKylie GolindangNo ratings yet
- Authorization Letter Jmm1Document1 pageAuthorization Letter Jmm1Kylie GolindangNo ratings yet
- Procuring and Sustaining ResourcesDocument17 pagesProcuring and Sustaining ResourcesKylie GolindangNo ratings yet
- Authorization Letter AumDocument1 pageAuthorization Letter AumKylie GolindangNo ratings yet
- Reading Passage 5Document10 pagesReading Passage 5Kylie GolindangNo ratings yet
- Reading Passage 7Document12 pagesReading Passage 7Kylie GolindangNo ratings yet
- Reading Passage 1Document11 pagesReading Passage 1Kylie GolindangNo ratings yet
- Reading Passage 1: You Should Spend About 20 Minutes On Questions 1-12, Which Are Based On Reading Passage 1 BelowDocument14 pagesReading Passage 1: You Should Spend About 20 Minutes On Questions 1-12, Which Are Based On Reading Passage 1 BelowKylie GolindangNo ratings yet
- Reading Passage 3Document13 pagesReading Passage 3Kylie GolindangNo ratings yet
- Do Not Write Anything On This Questionairre! Write Your Answer On The Answer Sheet Provided. Reading Passage 1Document11 pagesDo Not Write Anything On This Questionairre! Write Your Answer On The Answer Sheet Provided. Reading Passage 1Kylie GolindangNo ratings yet
- My Sleep OverDocument1 pageMy Sleep OverKylie GolindangNo ratings yet
- PH Protocol For Nephrotic SyndromeDocument4 pagesPH Protocol For Nephrotic Syndromeprachi100% (1)
- Assignment 3 - Asthma and Bronchiolitis - Case StudyDocument4 pagesAssignment 3 - Asthma and Bronchiolitis - Case StudyChaerin LeeNo ratings yet
- Surgical Skin Prep StandardsDocument19 pagesSurgical Skin Prep StandardsSyahri DzikriNo ratings yet
- Cancer CervixDocument7 pagesCancer Cervixkalpana gondipalliNo ratings yet
- What Is Aids Causing How Long Does HIV Take To Become AIDS Types of HIV Diagnoses Transmission Symptoms Curing (Treatments) Preventing of The DiseaseDocument11 pagesWhat Is Aids Causing How Long Does HIV Take To Become AIDS Types of HIV Diagnoses Transmission Symptoms Curing (Treatments) Preventing of The DiseaseAsha lakraNo ratings yet
- Lab Manual 1Document246 pagesLab Manual 1Harshan Isuru Kumara100% (1)
- Mrunal Mock Test #1 - NCERT 100 MCQs From Class 6, 8 & 10 PDFDocument20 pagesMrunal Mock Test #1 - NCERT 100 MCQs From Class 6, 8 & 10 PDFGauravKumarNo ratings yet
- Hepatitis Viruses Combination (Blood Borne Pathogens)Document51 pagesHepatitis Viruses Combination (Blood Borne Pathogens)Hosam GomaaNo ratings yet
- Somali-Praise and WorshipDocument159 pagesSomali-Praise and WorshipDr. A.L. and Joyce Gill100% (1)
- Common DOG Bite DiseasesDocument3 pagesCommon DOG Bite DiseaseskhurramNo ratings yet
- 1st Semester Lec 01 - Clin para General IntroductionDocument18 pages1st Semester Lec 01 - Clin para General IntroductionSofina JenpoNo ratings yet
- Cephalosporins - 1st Generation To 5th GenerationDocument4 pagesCephalosporins - 1st Generation To 5th GenerationDr. Sadaf khanNo ratings yet
- TRT2017 4920209Document12 pagesTRT2017 4920209ADVOCATE ASHUTOSH SHARMANo ratings yet
- Diagnostics 13 00220Document20 pagesDiagnostics 13 00220msworkbbhNo ratings yet
- Central Sterile Supply DepartmentDocument24 pagesCentral Sterile Supply DepartmentVikas DhyaniNo ratings yet
- WHO-PPL-Short Summary 25Feb-ET NM WHO PDFDocument7 pagesWHO-PPL-Short Summary 25Feb-ET NM WHO PDFRichard Caceda VizcondeNo ratings yet
- China Daily-2020-05-07 PDFDocument21 pagesChina Daily-2020-05-07 PDFJackZhangNo ratings yet
- 2nd Year SyllabusDocument24 pages2nd Year Syllabuspraveen MNo ratings yet
- Resume Zester HerpesDocument3 pagesResume Zester HerpesdiahayumustikaNo ratings yet
- Geneva DengueDocument168 pagesGeneva DengueangelaenjeliaNo ratings yet
- Hepatitis B and Pregnancy: An Underestimated Issue: 2009 John Wiley & Sons A/SDocument7 pagesHepatitis B and Pregnancy: An Underestimated Issue: 2009 John Wiley & Sons A/SFenny Noor AidaNo ratings yet
- Sexually Transmitted Diseases - Part 1: DR Clarissa ListerDocument20 pagesSexually Transmitted Diseases - Part 1: DR Clarissa Listerandreas kevinNo ratings yet
- 06-07-2020 PDFDocument99 pages06-07-2020 PDFThanup CseNo ratings yet
- SparganosisDocument21 pagesSparganosisJose Ho100% (1)
- National Safety and Quality Health Service Standards Guide For HospitalsDocument356 pagesNational Safety and Quality Health Service Standards Guide For HospitalsriskaNo ratings yet
- Cauti Prevention - UpdatedDocument25 pagesCauti Prevention - Updatedapi-340518242No ratings yet
- OCR BlueprintsSeries PediatricInfectiousDiseases2004ShahDocument237 pagesOCR BlueprintsSeries PediatricInfectiousDiseases2004ShahAnthonyJohanNo ratings yet
- SPEC3-1 Roots of Corruption - InfestationDocument60 pagesSPEC3-1 Roots of Corruption - InfestationBob WongNo ratings yet
- DR Beck01 PDFDocument30 pagesDR Beck01 PDFgonzalez1No ratings yet
- Diagnostic Assays & Instruments: Gold Standard Diagnostics Europe 2022 International CatalogueDocument28 pagesDiagnostic Assays & Instruments: Gold Standard Diagnostics Europe 2022 International CatalogueMentor KurshumliuNo ratings yet