You might also like
- Hemorrhage NCPDocument4 pagesHemorrhage NCPElishaNo ratings yet
- Infant Attachment NCPDocument2 pagesInfant Attachment NCPMary Hope BacutaNo ratings yet
- Drug Ang NCPDocument9 pagesDrug Ang NCPMelanie GaledoNo ratings yet
- NCP Dysfunctional Uterine BleedingDocument2 pagesNCP Dysfunctional Uterine BleedingDayan CabrigaNo ratings yet
- NCP Impaired SkinDocument2 pagesNCP Impaired Skinarjay2306_obcq100% (1)
- Altered Tissue Perfusion UteroplacentalDocument4 pagesAltered Tissue Perfusion UteroplacentalAlyNo ratings yet
- NCP OBDocument3 pagesNCP OBmikaela_magsinoNo ratings yet
- Ectopic PregnancyDocument2 pagesEctopic PregnancyRex Dave Guinoden100% (1)
- NCP: Acute GastroenteritisDocument3 pagesNCP: Acute GastroenteritishauteanicoleNo ratings yet
- NCP - Labor ActiveDocument4 pagesNCP - Labor ActiveKarizza Mae Celis100% (2)
- NCP Acute PainDocument3 pagesNCP Acute PainAngel HernandezNo ratings yet
- Actual Impairment of Skin Integrity in The Perineum Related To Episiotomy Wound Secondary To Normal Birth DeliveryDocument2 pagesActual Impairment of Skin Integrity in The Perineum Related To Episiotomy Wound Secondary To Normal Birth DeliveryNathalieCaracaNo ratings yet
- Ectopic Pregnancy: A Nursing Care Plan OnDocument12 pagesEctopic Pregnancy: A Nursing Care Plan OnajNo ratings yet
- NCP Gestational HypertensionDocument2 pagesNCP Gestational Hypertensionshila_glangNo ratings yet
- NCP Acute Pain OB Ward PDFDocument2 pagesNCP Acute Pain OB Ward PDFambiit25No ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainSheene Lysethea Sioteco AguilosNo ratings yet
- Assessment Diagnosis Rationale Planning Intervention Rationale EvaluationDocument3 pagesAssessment Diagnosis Rationale Planning Intervention Rationale EvaluationMark FernandezNo ratings yet
- 1 NCPDocument2 pages1 NCPAudrey Martin RañisesNo ratings yet
- Nursing Care PlanDocument6 pagesNursing Care PlanAnthea ValinoNo ratings yet
- Risk For Infection Related To Inadequate Primary Defenses: Broken SkinDocument2 pagesRisk For Infection Related To Inadequate Primary Defenses: Broken SkinReylan Garcia100% (8)
- NCP Actual and PotentialDocument4 pagesNCP Actual and PotentialKristian Karl Bautista Kiw-isNo ratings yet
- NCP-Risk For InfectionDocument2 pagesNCP-Risk For InfectionJea Joel Mendoza100% (1)
- Nursing Care PlanDocument2 pagesNursing Care PlanAbby Guiritan100% (1)
- Nursing Care Plan. LyksDocument3 pagesNursing Care Plan. LyksKiyla92No ratings yet
- Edited Risk For MaternalDocument2 pagesEdited Risk For MaternalElisha100% (1)
- Nursing Care Plan Assessment Diagnosis Planning Implementation Rationale EvaluationDocument1 pageNursing Care Plan Assessment Diagnosis Planning Implementation Rationale EvaluationMyrien BanaagNo ratings yet
- Nursing Diagnosis Background Study Inference Goals and Objectives Interventions Rationale EvaluationDocument5 pagesNursing Diagnosis Background Study Inference Goals and Objectives Interventions Rationale EvaluationAubrey SungaNo ratings yet
- Spinal Bifida Ncp-Impaired Physical MobilityDocument3 pagesSpinal Bifida Ncp-Impaired Physical MobilityNicole cuencos50% (2)
- FNCP ProperDocument3 pagesFNCP ProperSoniaMarieBalanayNo ratings yet
- Care Plan PostpartumDocument2 pagesCare Plan Postpartumteokie082483% (6)
- Risk For InfectionDocument3 pagesRisk For InfectionJennelyn BayleNo ratings yet
- Assessment Nursing Diagnoses Planning Implementation Rationale Evaluation Subjective Data: Short-Term GoalDocument2 pagesAssessment Nursing Diagnoses Planning Implementation Rationale Evaluation Subjective Data: Short-Term GoalMark oliver GonzalesNo ratings yet
- Body Weakness NCPDocument1 pageBody Weakness NCPArnold Christian QuilonNo ratings yet
- 5b - NCPDocument7 pages5b - NCPKelly Camero ÜNo ratings yet
- Nursing Care Plan For Client With Parent-Infant AttachmentDocument2 pagesNursing Care Plan For Client With Parent-Infant AttachmentThe Right WayNo ratings yet
- Assessment Diagnisis Planning Intervention Rationale Evaluation SubjectiveDocument2 pagesAssessment Diagnisis Planning Intervention Rationale Evaluation SubjectiveDanica Kate GalleonNo ratings yet
- College of Nursing: Rupture of Membrames On Full Term PrimigravidaDocument7 pagesCollege of Nursing: Rupture of Membrames On Full Term PrimigravidaJulia BanagodosNo ratings yet
- Nursing Care Plan For RabiesDocument1 pageNursing Care Plan For RabiesAngel VillamorNo ratings yet
- Ineffective Breastfeeding RT To Inadequate Milk Supply Secondary To Inverted NippleDocument3 pagesIneffective Breastfeeding RT To Inadequate Milk Supply Secondary To Inverted NippleKerny BasilioNo ratings yet
- NCP sLEEP DEPRIVATIONDocument4 pagesNCP sLEEP DEPRIVATIONArianna MabungaNo ratings yet
- NCP Post TermDocument2 pagesNCP Post TermFhairy Jhoy Rhayta100% (1)
- Readiness For Enhanced Health ManagementDocument6 pagesReadiness For Enhanced Health ManagementJIMENEZ, TRISHA MARIE D.No ratings yet
- NCP - Ineffective Airway ClearanceDocument4 pagesNCP - Ineffective Airway ClearanceKen RegalaNo ratings yet
- Nursing Care Plan - Spontaneous AbortionDocument2 pagesNursing Care Plan - Spontaneous Abortionderic100% (2)
- NCP For Caesarian Delivery (Breech Presentation)Document2 pagesNCP For Caesarian Delivery (Breech Presentation)Raymond BasiloniaNo ratings yet
- Nursingcrib Com NURSING CARE PLAN Spontaneous AbortionDocument2 pagesNursingcrib Com NURSING CARE PLAN Spontaneous AbortionMina RacadioNo ratings yet
- NCP MyomaDocument6 pagesNCP MyomaIzza Mae Ferrancol PastranaNo ratings yet
- NCP CSDocument9 pagesNCP CSFreida Marie PiczonNo ratings yet
- Episiotomy Wound NCPDocument2 pagesEpisiotomy Wound NCPnethcecilia90% (10)
- Cholecystectomy Nursing Care PlanDocument1 pageCholecystectomy Nursing Care PlanJor Garcia100% (1)
- NCP BreastfeedingDocument3 pagesNCP BreastfeedingLeo FrivaldoNo ratings yet
- NCP - Acute Pain Related To EdemaDocument2 pagesNCP - Acute Pain Related To EdemaChenime Añana0% (1)
- Acute Pain NCPDocument2 pagesAcute Pain NCPfaye-pamatmat-257080% (5)
- Methergine Drug StudyDocument1 pageMethergine Drug StudyMarlet N. OrtegaNo ratings yet
- Assessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation IndependentDocument4 pagesAssessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation IndependentJoseph Rodney de LeonNo ratings yet
- BDH NCP Medical FormDocument9 pagesBDH NCP Medical FormRegie CanoNo ratings yet
- NCPs For ParotidectomyDocument8 pagesNCPs For ParotidectomyAcohCChao100% (1)
- NCPs For ParotidectomyDocument12 pagesNCPs For ParotidectomyCarla Manaloto50% (2)
- Postoperative Phase 2021Document56 pagesPostoperative Phase 2021Jmarie Brillantes PopiocoNo ratings yet
- NCPDocument17 pagesNCPShayne Jessemae AlmarioNo ratings yet
- Laser Eye Surgery - HTTP WWW - Irishhealth.com ArticleDocument306 pagesLaser Eye Surgery - HTTP WWW - Irishhealth.com ArticleAziz ul HakeemNo ratings yet
- BHP Medis Ranap UgdDocument2 pagesBHP Medis Ranap UgdPuskesmas GembongNo ratings yet
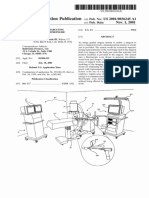
- Patent Application Publication (10) Pub. No.: US 2001/0036245 A1Document38 pagesPatent Application Publication (10) Pub. No.: US 2001/0036245 A1mohadeseNo ratings yet
- The Bariatric Surgery Patients Essential GuidebookDocument104 pagesThe Bariatric Surgery Patients Essential GuidebookJesus Pinto Elera100% (1)
- Mock 2Document40 pagesMock 2Syali Sasidharan100% (2)
- HUSNI ADAM - Jurnal Utama No.3Document3 pagesHUSNI ADAM - Jurnal Utama No.3Adam HusniNo ratings yet
- Trauma TriageDocument34 pagesTrauma TriageMonica FalconeNo ratings yet
- Biological Techniques Procedures and Methods - Asceptic Technique1Document39 pagesBiological Techniques Procedures and Methods - Asceptic Technique1Iphone. ColasticNo ratings yet
- CritiqueDocument2 pagesCritiqueJerecel Gapi VigoNo ratings yet
- Principles of Dentoalveolar ExtractionsDocument143 pagesPrinciples of Dentoalveolar ExtractionsRogleva RoskaNo ratings yet
- Program EPSRC FINALDocument13 pagesProgram EPSRC FINALCorneliu ComanNo ratings yet
- Seroma InglesDocument13 pagesSeroma InglesMary Alejandra Loayza PatiñoNo ratings yet
- OrthoNeuro Neurologist Dr. Martin Taylor Enrolls First Patient in The United States and Australia For New Parkinson's Phase 3 Research TrialDocument2 pagesOrthoNeuro Neurologist Dr. Martin Taylor Enrolls First Patient in The United States and Australia For New Parkinson's Phase 3 Research TrialPR.comNo ratings yet
- 2018 Surgical Rescue in Medical PatientsDocument11 pages2018 Surgical Rescue in Medical PatientsgiseladlrNo ratings yet
- HMRM RECORD DoccDocument13 pagesHMRM RECORD DoccBharath BeeNo ratings yet
- Medoral 21 E696Document7 pagesMedoral 21 E696andreeaNo ratings yet
- 2010Document3 pages2010Harshitha KhambampatiNo ratings yet
- HospitalAdministration 2Document13 pagesHospitalAdministration 2JairAntonAtuncarNo ratings yet
- International Journal of Surgery Open: Mengesha Dessie AlleneDocument5 pagesInternational Journal of Surgery Open: Mengesha Dessie AllenebejarhasanNo ratings yet
- Management of The Patient With A Burn InjuryDocument43 pagesManagement of The Patient With A Burn InjuryAshraf HusseinNo ratings yet
- FJLGKKJFBVN, KhkdsljhlkxcidhlisxhfkjdbfhlkjdsbhflkudshljxzhbDocument931 pagesFJLGKKJFBVN, KhkdsljhlkxcidhlisxhfkjdbfhlkjdsbhflkudshljxzhbTalal HajNo ratings yet
- CPHQ PrepDocument50 pagesCPHQ PrepTOBIN6319_39572798689% (9)
- Procedure Rationale RD 1 2 PEDocument7 pagesProcedure Rationale RD 1 2 PEKyla CalzadoNo ratings yet
- P2 Long Exam A 15 Block 3 Funda Lecture PDFDocument25 pagesP2 Long Exam A 15 Block 3 Funda Lecture PDFryllerylle05No ratings yet
- 30-60-90 - Plan Sample - Medical Sales RepDocument5 pages30-60-90 - Plan Sample - Medical Sales RepTahar Belgaied HassineNo ratings yet
- Recommendations For Infection Control For The Practice of AnesthesiologyDocument86 pagesRecommendations For Infection Control For The Practice of AnesthesiologyAhmed MostafaNo ratings yet
- Certificate of InsuranceDocument31 pagesCertificate of InsurancebenNo ratings yet
- Vision & Mission: Healthc Are Solution GroupDocument16 pagesVision & Mission: Healthc Are Solution GroupFajar Pandu WijayaNo ratings yet
- AOI Kerala Mid-Term Conference 2018 BrochureDocument5 pagesAOI Kerala Mid-Term Conference 2018 BrochureSUJEET KUMARNo ratings yet