You might also like
- Nursing Upper Gi BleedingDocument23 pagesNursing Upper Gi BleedingLord Pozak Miller100% (3)
- Artery-First Approaches To Pancreatoduodenectomy BJS 2011Document9 pagesArtery-First Approaches To Pancreatoduodenectomy BJS 2011Roberto Hernandez100% (1)
- Breast Cancer PowerpointDocument13 pagesBreast Cancer PowerpointCara DeaNo ratings yet
- Lung Cancer Presentation FinalDocument48 pagesLung Cancer Presentation Finalراس زهد ارفنندNo ratings yet
- Dance - Davis Intubated Ureterotomy in A Child - 05202016Document27 pagesDance - Davis Intubated Ureterotomy in A Child - 05202016sirrfsNo ratings yet
- Quantec 02Document7 pagesQuantec 02onco100% (1)
- Fast Facts: Cholangiocarcinoma: Diagnostic and therapeutic advances are improving outcomesFrom EverandFast Facts: Cholangiocarcinoma: Diagnostic and therapeutic advances are improving outcomesNo ratings yet
- Laparoscopic Resection of Rectal CancerDocument4 pagesLaparoscopic Resection of Rectal CancerhoangducnamNo ratings yet
- Sentinel Lymph Node ConceptDocument27 pagesSentinel Lymph Node ConceptKarthikeyan RadhakrishnanNo ratings yet
- Hepatocellular Carcinoma: Review ArticleDocument13 pagesHepatocellular Carcinoma: Review ArticleAnnagiulia Gramenzi100% (2)
- Artery First Approach To Pancreatic Cancer Resection A Review of The Evidence For BenefitDocument3 pagesArtery First Approach To Pancreatic Cancer Resection A Review of The Evidence For BenefitFlaviu Ionuț FaurNo ratings yet
- Colorectal Cancer 1Document71 pagesColorectal Cancer 1Anupam SisodiaNo ratings yet
- Subtotal Cholecystectomy-''Fenestrating'' Vs ''Reconstituting'' Subtypes and The Prevention of Bile Duct Injury - Definition of The Optimal Procedure In  Difficult Operative ConditionsDocument8 pagesSubtotal Cholecystectomy-''Fenestrating'' Vs ''Reconstituting'' Subtypes and The Prevention of Bile Duct Injury - Definition of The Optimal Procedure In  Difficult Operative ConditionsBolivar Isea100% (1)
- Sentinal Lymph Node BiopsyDocument12 pagesSentinal Lymph Node BiopsySahirNo ratings yet
- In Service Exam For Breast DR Paul BalisiDocument11 pagesIn Service Exam For Breast DR Paul BalisiAmiel Francisco ReyesNo ratings yet
- NRG Protocol Radiation Therapy Template - GYN - Endometrial Cancer - FinalDocument12 pagesNRG Protocol Radiation Therapy Template - GYN - Endometrial Cancer - FinalarifpharmjuNo ratings yet
- Thymoma: Dr. Ravi Gadani MS, FmasDocument31 pagesThymoma: Dr. Ravi Gadani MS, FmasRaviNo ratings yet
- ILRT Dr. Sarbani-1 PDFDocument48 pagesILRT Dr. Sarbani-1 PDFdurgesh kumar100% (1)
- Rectal Cancer Contouring Guide: Econtour TeamDocument29 pagesRectal Cancer Contouring Guide: Econtour TeamRonna Marie Vijar PamalandongNo ratings yet
- Trimodality Therapy in Bladder CancerDocument12 pagesTrimodality Therapy in Bladder CancerStirNo ratings yet
- The Lecture: "Tumours of The Mammary Gland."Document21 pagesThe Lecture: "Tumours of The Mammary Gland."top theNo ratings yet
- Brachytherapy in Cancer CervixDocument65 pagesBrachytherapy in Cancer CervixSatyesh NadellaNo ratings yet
- Diagnostic Tools in ObgynDocument27 pagesDiagnostic Tools in ObgynHenok Y KebedeNo ratings yet
- EAU ESUR ESTRO SIOG Guidelines On Prostate Cancer Large Text V2Document145 pagesEAU ESUR ESTRO SIOG Guidelines On Prostate Cancer Large Text V2DellaNo ratings yet
- Management of The Pancreatic Remnant During Whipple OperationDocument4 pagesManagement of The Pancreatic Remnant During Whipple OperationYacine Tarik Aizel100% (1)
- PET CT in Oncology Integration Into Clin PDFDocument10 pagesPET CT in Oncology Integration Into Clin PDFZafr O'Connell100% (1)
- "Management of Liver Secondaries": Dr. MukeshDocument36 pages"Management of Liver Secondaries": Dr. MukeshSasi Kumar100% (1)
- Appendiceal Cancer: - 1% of Appendectomies Contain CancerDocument28 pagesAppendiceal Cancer: - 1% of Appendectomies Contain CancerRajendra SoniNo ratings yet
- Locally Advanced Breast CarcinomaDocument31 pagesLocally Advanced Breast Carcinomaapi-3701915100% (1)
- AmputationDocument51 pagesAmputationStar CruiseNo ratings yet
- Vascular Presentation - Visceral Artery Aneurysms - MCGDocument22 pagesVascular Presentation - Visceral Artery Aneurysms - MCGYasir BouchiNo ratings yet
- Superior Vena Cava Obstruction: Aditya Rachakonda, PGY4 December 8, 2014Document35 pagesSuperior Vena Cava Obstruction: Aditya Rachakonda, PGY4 December 8, 2014jhk0428No ratings yet
- 05 Birads Us Reporting Acr 2013Document12 pages05 Birads Us Reporting Acr 2013shilacorinaNo ratings yet
- Colorectal Screening AlgorithmDocument12 pagesColorectal Screening Algorithmsavvy_as_98No ratings yet
- APBI Journal Club PowerPointDocument20 pagesAPBI Journal Club PowerPointRegan Ward HimeNo ratings yet
- Radiation Therapy Case Study 2Document11 pagesRadiation Therapy Case Study 2api-278170649No ratings yet
- Nuclear OncologyDocument33 pagesNuclear OncologyOvguOzenliNo ratings yet
- 10 Intraoperative RadiotherapyDocument11 pages10 Intraoperative RadiotherapyDgek LondonNo ratings yet
- 7.30.08 Volk. Mesenteric IschemiaDocument16 pages7.30.08 Volk. Mesenteric Ischemiaowcordal7297No ratings yet
- Prostate Radiotherapy - Current Standards and Future DirectionsDocument40 pagesProstate Radiotherapy - Current Standards and Future Directionsvikram_bansal84No ratings yet
- Role of Radiotherapy in Carcinoma CervixDocument68 pagesRole of Radiotherapy in Carcinoma CervixInsighte Behavioral CareNo ratings yet
- Radiotherapy in Penile Carcinoma: Dr. Ayush GargDocument32 pagesRadiotherapy in Penile Carcinoma: Dr. Ayush GargMohammad Mahfujur RahmanNo ratings yet
- SAGES Gallbladder CBDDocument54 pagesSAGES Gallbladder CBDSAGESWeb100% (1)
- Imaging in Vascular SurgeryDocument33 pagesImaging in Vascular Surgerydrzalie70100% (1)
- Breast ReviewDocument147 pagesBreast Reviewlovelots1234100% (1)
- Oncoplastic and Reconstructive BreastDocument14 pagesOncoplastic and Reconstructive BreastYefry Onil Santana Marte100% (1)
- Carcinoma Penis Management: Dr. Lilamani Rajthala MS Resident Moderator: Dr. Samir ShresthaDocument63 pagesCarcinoma Penis Management: Dr. Lilamani Rajthala MS Resident Moderator: Dr. Samir ShresthaBibek GhimireNo ratings yet
- Matthew Kilmurry, M.D. St. Mary's General Hospital Grand River HospitalDocument29 pagesMatthew Kilmurry, M.D. St. Mary's General Hospital Grand River HospitalSalmanArifNo ratings yet
- Open Jejunostomy: Steven J. Hughes, MD and A. James Moser, MDDocument8 pagesOpen Jejunostomy: Steven J. Hughes, MD and A. James Moser, MDAndres BernalNo ratings yet
- BranchialCleftCyst GerDocument36 pagesBranchialCleftCyst GerDrsreeram Valluri100% (1)
- An Updated Review of Cystic Hepatic LesionsDocument8 pagesAn Updated Review of Cystic Hepatic LesionsMayerlin CalvacheNo ratings yet
- Management of High Grade Bladder Cancer & Carcinoma in SituDocument26 pagesManagement of High Grade Bladder Cancer & Carcinoma in SituSakuntalaPalankiNo ratings yet
- Preparing Severely Jaundiced Patient For SurgeryDocument2 pagesPreparing Severely Jaundiced Patient For Surgerylentini@maltanet.netNo ratings yet
- Understanding BrachytherapyDocument28 pagesUnderstanding Brachytherapyqwertu132No ratings yet
- Mucoepidermoid Carcinomaof The External Auditory Canal (Eac)Document4 pagesMucoepidermoid Carcinomaof The External Auditory Canal (Eac)IJAR JOURNALNo ratings yet
- Review: Benjamin O Anderson, Riccardo Masetti, Melvin J SilversteinDocument13 pagesReview: Benjamin O Anderson, Riccardo Masetti, Melvin J SilversteinsanineseinNo ratings yet
- Pancreatic CancerDocument4 pagesPancreatic Cancersdf100% (1)
- Esophageal CancerDocument43 pagesEsophageal Cancerapi-19641337No ratings yet
- Intraoperative Irradiation Techniques and ResultsDocument533 pagesIntraoperative Irradiation Techniques and ResultsTELLY GONZALO ROMERO BRIOSONo ratings yet
- Mammography - Procedure, Test, Pain, Time, Types, Risk, Cancer, RateDocument4 pagesMammography - Procedure, Test, Pain, Time, Types, Risk, Cancer, RateMassimo RiserboNo ratings yet
- A Thesis ProtocolDocument29 pagesA Thesis ProtocolMelvin JohnNo ratings yet
- Pilar Cyst With CrystalsDocument2 pagesPilar Cyst With CrystalsDeba P SarmaNo ratings yet
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Document3 pagesAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaNo ratings yet
- Accessory TragusDocument3 pagesAccessory TragusDeba P SarmaNo ratings yet
- Acantholytic Dermatosis With DyskeratosisDocument11 pagesAcantholytic Dermatosis With DyskeratosisDeba P SarmaNo ratings yet
- Acantholytic Solar Keratosis, M 67, Forehead PDFDocument6 pagesAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaNo ratings yet
- Results of Search in Google Scholar On 'Deba P Sarma'Document28 pagesResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaNo ratings yet
- Acantholytic Actinic KeratosisDocument4 pagesAcantholytic Actinic KeratosisDeba P SarmaNo ratings yet
- Acantholytic Bullous DiseaseDocument4 pagesAcantholytic Bullous DiseaseDeba P SarmaNo ratings yet
- Acantholytic Acanthoma. M 60, ScrotumDocument8 pagesAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaNo ratings yet
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Document6 pagesBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaNo ratings yet
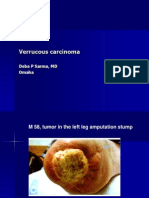
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDocument7 pagesVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaNo ratings yet
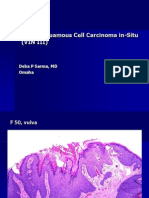
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDocument6 pagesVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaNo ratings yet
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDocument7 pagesXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaNo ratings yet
- Xanthogranuloma, M 30, Right ElbowDocument4 pagesXanthogranuloma, M 30, Right ElbowDeba P SarmaNo ratings yet
- Verrucous Epidermal Nevus. F 43, ScalpDocument4 pagesVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaNo ratings yet
- Xanthogranuloma PPT DSDocument9 pagesXanthogranuloma PPT DSDeba P SarmaNo ratings yet
- Verrucous Carcinoma of The Foot, M 63, Left FootDocument8 pagesVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- Verruca Vulgaris., M 22.,PPTDocument2 pagesVerruca Vulgaris., M 22.,PPTDeba P SarmaNo ratings yet
- Teaching Plan About Conjunctivitis: Haemophilus InfluenzaeDocument3 pagesTeaching Plan About Conjunctivitis: Haemophilus InfluenzaeJanaica Juan100% (1)
- Felicias Resume 1Document1 pageFelicias Resume 1api-357153848No ratings yet
- 9000 One Liner GK PDF in Hindi (For More Book - WWW - Gktrickhindi.com)Document25 pages9000 One Liner GK PDF in Hindi (For More Book - WWW - Gktrickhindi.com)Ashish gautam100% (1)
- Periodontal Plastic SurgeryDocument5 pagesPeriodontal Plastic Surgeryudhai170819No ratings yet
- Autoimmune Mash - Up FinalDocument38 pagesAutoimmune Mash - Up Finalapi-546809761No ratings yet
- Raasn October NewsletterDocument6 pagesRaasn October Newsletterapi-231055558No ratings yet
- Journal B.cereus With PCR 2017Document10 pagesJournal B.cereus With PCR 2017deryl sepradanaNo ratings yet
- The Accidental AddictsDocument6 pagesThe Accidental AddictsnorthandsouthnzNo ratings yet
- Hybrid Hues 2008Document196 pagesHybrid Hues 2008Kulsharma100% (1)
- Hap-1 Question Paper 2018-19 1st SemesterDocument1 pageHap-1 Question Paper 2018-19 1st SemesterLavanya Tanguturi yellaNo ratings yet
- Surgical Correction Subglottic Stenosis of The Larynx: AnnoldDocument6 pagesSurgical Correction Subglottic Stenosis of The Larynx: Annoldcanndy202No ratings yet
- Bell's Palsy Treatments & Medications - SingleCareDocument11 pagesBell's Palsy Treatments & Medications - SingleCareRoxan PacsayNo ratings yet
- Orthotic/Prosthetic Referral Form: Dispensing RX: Please Evaluate and Treat Patient With The Following DeviceDocument1 pageOrthotic/Prosthetic Referral Form: Dispensing RX: Please Evaluate and Treat Patient With The Following DeviceKelly Roberts WiggenNo ratings yet
- OT HoppysAppReviewDocument1 pageOT HoppysAppReviewIris De La CalzadaNo ratings yet
- OHS-TBT-010 - Types of Hazards - 1Document1 pageOHS-TBT-010 - Types of Hazards - 1Tony NhabangaNo ratings yet
- Trends of Violence Against Healthcare by ShaheerDocument9 pagesTrends of Violence Against Healthcare by ShaheerShaheer zia100% (1)
- Personal Accident Claim Form: Particulars of Insured (Company / Individual)Document2 pagesPersonal Accident Claim Form: Particulars of Insured (Company / Individual)Robbie Chan100% (1)
- First Aid TrainingDocument202 pagesFirst Aid TrainingTheFreeSpiritNo ratings yet
- CHP 11 Moderate Nonskeletal Problems in Preadolescent ChildrenDocument6 pagesCHP 11 Moderate Nonskeletal Problems in Preadolescent ChildrenJack Pai33% (3)
- Attenuation AssignmentDocument15 pagesAttenuation Assignmentapi-336647605No ratings yet
- What Are Thrombosed External Hemorrhoids?Document3 pagesWhat Are Thrombosed External Hemorrhoids?Hanine HassanNo ratings yet
- Final Resume Package Douglas ShawDocument3 pagesFinal Resume Package Douglas Shawapi-347691125No ratings yet
- Post-Cardiac Arrest Therapeutic Hypothermia Targeted Temperature Manangement (TTM) Quick SheetDocument3 pagesPost-Cardiac Arrest Therapeutic Hypothermia Targeted Temperature Manangement (TTM) Quick SheetkimberlyNo ratings yet
- Medical Image ProcessingDocument24 pagesMedical Image ProcessingInjeti satish kumarNo ratings yet
- Percakapan BHS Ingg 1-5 - OciDocument30 pagesPercakapan BHS Ingg 1-5 - OciYetty LasmiNo ratings yet
- EYE MCQ Uploaded by Hafiz BilalDocument2 pagesEYE MCQ Uploaded by Hafiz BilalMohammad Jamal NasirNo ratings yet
- Uniformity of Dosage UnitsDocument5 pagesUniformity of Dosage UnitsJai MurugeshNo ratings yet
- SA Anesthesia Drug Dosages 2022Document3 pagesSA Anesthesia Drug Dosages 2022KRLITHIU Borja100% (1)
- ICD X Kes HajiDocument2 pagesICD X Kes Hajiyasin_rsdk67% (3)