You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Characteristics and Elements of A Business Letter Characteristics of A Business LetterDocument3 pagesCharacteristics and Elements of A Business Letter Characteristics of A Business LetterPamela Galang100% (1)
- Garner Fructis ShampooDocument3 pagesGarner Fructis Shampooyogesh0794No ratings yet
- Lab Report FormatDocument2 pagesLab Report Formatapi-276658659No ratings yet
- General First Aid QuizDocument3 pagesGeneral First Aid QuizLucy KiturNo ratings yet
- GeM Bidding 2920423 - 2Document4 pagesGeM Bidding 2920423 - 2Sulvine CharlieNo ratings yet
- STD Symptoms, Causes and PreventionDocument3 pagesSTD Symptoms, Causes and PreventionSakshi TyagiNo ratings yet
- 3 QDocument2 pages3 QJerahmeel CuevasNo ratings yet
- Research Course Outline For Resarch Methodology Fall 2011 (MBA)Document3 pagesResearch Course Outline For Resarch Methodology Fall 2011 (MBA)mudassarramzanNo ratings yet
- Chapter 1Document30 pagesChapter 1Sneha AgarwalNo ratings yet
- XSI Public Indices Ocean Freight - January 2021Document7 pagesXSI Public Indices Ocean Freight - January 2021spyros_peiraiasNo ratings yet
- Runner Cs-47 Link Rev-2 27-09-10Document29 pagesRunner Cs-47 Link Rev-2 27-09-10bocko74No ratings yet
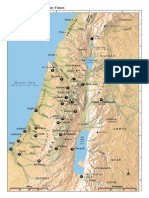
- Israel Bible MapDocument1 pageIsrael Bible MapMoses_JakkalaNo ratings yet
- English FinalDocument321 pagesEnglish FinalManuel Campos GuimeraNo ratings yet
- Research 2020.21 Outline PDFDocument12 pagesResearch 2020.21 Outline PDFCharles MaherNo ratings yet
- Dhikr or Zikr or Remembrance of AllahDocument27 pagesDhikr or Zikr or Remembrance of AllahMd. Naim KhanNo ratings yet
- ICE Learned Event DubaiDocument32 pagesICE Learned Event DubaiengkjNo ratings yet
- Hac 1001 NotesDocument56 pagesHac 1001 NotesMarlin MerikanNo ratings yet
- All About Linux SignalsDocument17 pagesAll About Linux SignalsSK_shivamNo ratings yet
- Philippine Association of Service Exporters vs Drilon Guidelines on Deployment BanDocument1 pagePhilippine Association of Service Exporters vs Drilon Guidelines on Deployment BanRhev Xandra AcuñaNo ratings yet
- Shilajit The Panacea For CancerDocument48 pagesShilajit The Panacea For Cancerliving63100% (1)
- Organizational CultureDocument76 pagesOrganizational Culturenaty fishNo ratings yet
- Cambridge IGCSE: 0500/12 First Language EnglishDocument16 pagesCambridge IGCSE: 0500/12 First Language EnglishJonathan ChuNo ratings yet
- Agriculture Term Paper TopicsDocument5 pagesAgriculture Term Paper Topicsfuhukuheseg2100% (1)
- Surah Al A'araf (7:74) - People of ThamudDocument2 pagesSurah Al A'araf (7:74) - People of ThamudMuhammad Awais TahirNo ratings yet
- Life Pre-Intermediate Writing Worksheet Units 3&4Document4 pagesLife Pre-Intermediate Writing Worksheet Units 3&4SabrinaNo ratings yet
- Iso 1964 1987Document11 pagesIso 1964 1987Dina ANDRIAMAHEFAHERYNo ratings yet
- Effectiveness of Laundry Detergents and Bars in Removing Common StainsDocument9 pagesEffectiveness of Laundry Detergents and Bars in Removing Common StainsCloudy ClaudNo ratings yet
- Total Product Marketing Procedures: A Case Study On "BSRM Xtreme 500W"Document75 pagesTotal Product Marketing Procedures: A Case Study On "BSRM Xtreme 500W"Yasir Alam100% (1)
- Diagnosis of Dieback Disease of The Nutmeg Tree in Aceh Selatan, IndonesiaDocument10 pagesDiagnosis of Dieback Disease of The Nutmeg Tree in Aceh Selatan, IndonesiaciptaNo ratings yet
- Ds 1Document8 pagesDs 1michaelcoNo ratings yet