You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Planning Who We Are 1 2Document6 pagesPlanning Who We Are 1 2api-325889732100% (1)
- AG2018 OfficialResultBook Artistic Gymnastics v1.0Document146 pagesAG2018 OfficialResultBook Artistic Gymnastics v1.0De TrilekNo ratings yet
- What Is Physical ActivityDocument1 pageWhat Is Physical ActivityRosaAlyannaAntoninoNo ratings yet
- FIG Apparatus World Cup 2024 BAKU Nominative-1Document4 pagesFIG Apparatus World Cup 2024 BAKU Nominative-1Dana DanaNo ratings yet
- ISO Fit Mega ProgramDocument15 pagesISO Fit Mega Programdragos88% (8)
- Latihan Mingguan Lompat JauhDocument2 pagesLatihan Mingguan Lompat JauhmanrunnerNo ratings yet
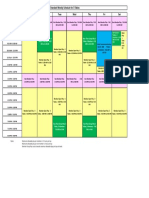
- Standard Weekly Billiard Schedule-2020 Version 2Document1 pageStandard Weekly Billiard Schedule-2020 Version 2lannett40No ratings yet
- LinksDocument2 pagesLinksAlvaro Diaz CanalesNo ratings yet
- Energy System DevelopmentDocument17 pagesEnergy System DevelopmentjhomalynNo ratings yet
- Lesson345.67 PEH John Andrei AlcantaraDocument15 pagesLesson345.67 PEH John Andrei AlcantaraMiguel, Nathaniel T.No ratings yet
- Kettlebell Workout Booklet: 23 Strength, Power & Conditioning CircuitsDocument18 pagesKettlebell Workout Booklet: 23 Strength, Power & Conditioning CircuitsJose Martinez100% (1)
- (1877) Practical Training For Running, Walking, Rowing, Wrestling, Boxing, Jumping, and All Kinds of Athletic Feats - Ed JamesDocument128 pages(1877) Practical Training For Running, Walking, Rowing, Wrestling, Boxing, Jumping, and All Kinds of Athletic Feats - Ed JamesSamurai_Chef100% (4)
- MetsDocument2 pagesMetssupreme_bangirasNo ratings yet
- Old School Iron Workouts Month 2 InkSaverDocument15 pagesOld School Iron Workouts Month 2 InkSaverNick Konstantopoulos100% (3)
- List of Attendees for the Three Day Sports Officiating Seminar-WorkshopDocument2 pagesList of Attendees for the Three Day Sports Officiating Seminar-WorkshopWynnZhruhMatulinaNo ratings yet
- Limbs of Astanga Yoga: Section I - 3.28.1-12 Kapila Describes TheDocument4 pagesLimbs of Astanga Yoga: Section I - 3.28.1-12 Kapila Describes TheLeena PurohitNo ratings yet
- General Strength & Conditioning Programme For Boxing: Overhead Walking LungesDocument3 pagesGeneral Strength & Conditioning Programme For Boxing: Overhead Walking LungesShawn ValentinoNo ratings yet
- Advanced muscle growth techniquesDocument40 pagesAdvanced muscle growth techniquestpNo ratings yet
- NCC - Ncmetcon (10 24 22)Document1 pageNCC - Ncmetcon (10 24 22)azizNo ratings yet
- Juggernaut Method Instructions:: Cycle 1Document9 pagesJuggernaut Method Instructions:: Cycle 1Bautista Martinez AngelloNo ratings yet
- Muscle Mass Weight ProgramDocument2 pagesMuscle Mass Weight ProgramWes BlackNo ratings yet
- M S T I S P G: Aximal Trength Raining Mproves Trength Erformance in RapplersDocument7 pagesM S T I S P G: Aximal Trength Raining Mproves Trength Erformance in Rapplersok okNo ratings yet
- Workout Program Summary 2024-02-03Document4 pagesWorkout Program Summary 2024-02-03zybriel.benal.jhsNo ratings yet
- PEDocument13 pagesPELovelyn BaclaoNo ratings yet
- Mock MCQ L1 Ch2,3 PDFDocument11 pagesMock MCQ L1 Ch2,3 PDFJyotsna Gupta100% (1)
- May 2018 Workout PlanDocument3 pagesMay 2018 Workout PlanRian DewantoNo ratings yet
- AerobicsDocument16 pagesAerobicsNick PalmNo ratings yet
- YogaDocument21 pagesYogaJaypee CancejoNo ratings yet
- Circuit TrainingDocument4 pagesCircuit TrainingJan Alan RosimoNo ratings yet
- Psychophysiologic Effects of Hatha Yoga On Musculoskeletal and Cardiopulmonary Function: A Literature ReviewDocument17 pagesPsychophysiologic Effects of Hatha Yoga On Musculoskeletal and Cardiopulmonary Function: A Literature ReviewNi Made Wirastuti ShantiNo ratings yet