You might also like
- Anabolic-androgenic steroids – risks and testing in sportsDocument4 pagesAnabolic-androgenic steroids – risks and testing in sportsWagen WerksNo ratings yet
- Steroid University: Course SyllabusDocument3 pagesSteroid University: Course SyllabusJavelin JohnasNo ratings yet
- Anabolic SteroidsDocument11 pagesAnabolic SteroidsRichard Limas83% (6)
- Anabolic Steroid Cycles: An Experts Guide To Optimum Use Testosterone: Sprint or Marathon?Document5 pagesAnabolic Steroid Cycles: An Experts Guide To Optimum Use Testosterone: Sprint or Marathon?mehrdad_4450% (2)
- List of Anabolic SteroidDocument21 pagesList of Anabolic SteroidJohn EdokawabataNo ratings yet
- Human Anatomy and PhysiologyDocument136 pagesHuman Anatomy and PhysiologyLuis Margarejo91% (11)
- The Massive Fraud Behind HIV Tests by Jon Rappoport PDFDocument9 pagesThe Massive Fraud Behind HIV Tests by Jon Rappoport PDFDan Bo100% (2)
- Definition of PharmacognosyDocument5 pagesDefinition of Pharmacognosysyeda khadijaNo ratings yet
- Ergogenic Aids A Review of Basic Science, Performance, Side Effects, and Status in Sports PDFDocument11 pagesErgogenic Aids A Review of Basic Science, Performance, Side Effects, and Status in Sports PDFRuben CapelaNo ratings yet
- Qku3093 Sports Nutrition NotesDocument19 pagesQku3093 Sports Nutrition NotesAizat Farhan100% (1)
- Growing Young PDF EbookDocument155 pagesGrowing Young PDF Ebooktudor11111100% (1)
- Weekly Home Learning Plan Science 8 Quarter 4, Week 3, June 21-25, 2021Document2 pagesWeekly Home Learning Plan Science 8 Quarter 4, Week 3, June 21-25, 2021kaycin DuzonNo ratings yet
- Steroid Research Paper ThesisDocument4 pagesSteroid Research Paper Thesissandrawoodtopeka100% (2)
- Anabolic Steroid: 1 List of Anabolic SteroidsDocument21 pagesAnabolic Steroid: 1 List of Anabolic SteroidsZiedTrikiNo ratings yet
- How Are AAS Abused?: AAS and Mental HealthDocument5 pagesHow Are AAS Abused?: AAS and Mental HealthAdrian Orlando HermoNo ratings yet
- Methandienone (Dianabol)Document4 pagesMethandienone (Dianabol)Dianabol5No ratings yet
- Prospective Echocardiographic Assessment of Androgenic-Anabolic Steroids Effects On Cardiac Structure and Function in Strength Athletes.Document8 pagesProspective Echocardiographic Assessment of Androgenic-Anabolic Steroids Effects On Cardiac Structure and Function in Strength Athletes.Waleed El-HawarryNo ratings yet
- Team 8 Official StatementDocument4 pagesTeam 8 Official StatementNicole ChloéNo ratings yet
- Anabolic Androgenic Steroid (AAS) Abuse: Not Only An Elite Performance Issue?Document2 pagesAnabolic Androgenic Steroid (AAS) Abuse: Not Only An Elite Performance Issue?Sita PrasidaNo ratings yet
- Steroid Research Paper ConclusionDocument4 pagesSteroid Research Paper Conclusiongw2cgcd9100% (1)
- Effect of Testosterone Boosters On Body Functions: Case ReportDocument6 pagesEffect of Testosterone Boosters On Body Functions: Case ReportDeepak SinghNo ratings yet
- Testesterone in Young MenDocument10 pagesTestesterone in Young MenPeachesOrangesApplesNo ratings yet
- Steroid Abuse Research Paper OutlineDocument7 pagesSteroid Abuse Research Paper Outlineafnkddsqagodlh100% (1)
- Steroids Research Paper OutlineDocument8 pagesSteroids Research Paper Outlinexoopgxplg100% (1)
- Research Paper On Steroids and AthletesDocument7 pagesResearch Paper On Steroids and Athletesfvfzfa5d100% (1)
- 2008 Anabolic Steroid UseDocument22 pages2008 Anabolic Steroid UseAlbert JacksonNo ratings yet
- Wilborn 20 Et 20 Al 20 IJSNEM202010Document9 pagesWilborn 20 Et 20 Al 20 IJSNEM202010Boris ColovicNo ratings yet
- Anabolic Steroids Research Paper OutlineDocument4 pagesAnabolic Steroids Research Paper Outlineefe6zst5100% (1)
- Abuse of Anabolic Steroids: A Dangerous Indulgence: SciencedirectDocument6 pagesAbuse of Anabolic Steroids: A Dangerous Indulgence: SciencedirectTiago FernandesNo ratings yet
- Research Paper On Anabolic SteroidsDocument4 pagesResearch Paper On Anabolic Steroidsgw131adsNo ratings yet
- Effects of Steroids Research PaperDocument6 pagesEffects of Steroids Research Paperfvhwd4yj100% (1)
- Anabolic Steroids in Athetics - How Well Do They Work and How DangerousDocument8 pagesAnabolic Steroids in Athetics - How Well Do They Work and How DangerousDiego CarletiNo ratings yet
- Experimental Physiology - 2022 - Cardaci - LGD 4033 and MK 677 Use Impacts Body Composition Circulating Biomarkers andDocument10 pagesExperimental Physiology - 2022 - Cardaci - LGD 4033 and MK 677 Use Impacts Body Composition Circulating Biomarkers andAshwin nambiarNo ratings yet
- Anabolic Androgenic SteroidsDocument9 pagesAnabolic Androgenic SteroidsSuzzanaNo ratings yet
- Research Paper On Steroids in SportsDocument4 pagesResearch Paper On Steroids in Sportsfys374dr100% (1)
- Age-Related Hormonal Adaptations, Muscle Circumference and Strength Development With 8 Weeks Moderate Intensity Resistance TrainingDocument6 pagesAge-Related Hormonal Adaptations, Muscle Circumference and Strength Development With 8 Weeks Moderate Intensity Resistance TrainingJuan Ricardo Sandoval SalcedoNo ratings yet
- Research Paper Topics On Steroids in SportsDocument4 pagesResearch Paper Topics On Steroids in Sportsgw155nah100% (1)
- Research Proposal 1Document5 pagesResearch Proposal 1hegij80723No ratings yet
- Steroids Research PaperDocument7 pagesSteroids Research Paperafeawldza100% (1)
- Testosterone Dose-Response Relationships in Healthy Young MenDocument6 pagesTestosterone Dose-Response Relationships in Healthy Young MenfrankiesdumpsterNo ratings yet
- Anabolic Steroids Research PaperDocument6 pagesAnabolic Steroids Research Paperfzgzygnp100% (1)
- Conclusion For Research Paper On SteroidsDocument6 pagesConclusion For Research Paper On Steroidsafeaudffu100% (1)
- The Development of Multiple Drug Use Amo PDFDocument10 pagesThe Development of Multiple Drug Use Amo PDFDanijel DamnjanovicNo ratings yet
- AAEs and PsychyatricsDocument10 pagesAAEs and PsychyatricsJorge FernándezNo ratings yet
- CXXXXXXXDocument11 pagesCXXXXXXXStella IsbiantoNo ratings yet
- Synthesized Muscle: Skepticism About Performance Enhancing Drugs in SportsDocument7 pagesSynthesized Muscle: Skepticism About Performance Enhancing Drugs in Sportsapi-341215669No ratings yet
- Final Paper - Anabolic SteroidsDocument8 pagesFinal Paper - Anabolic Steroidsasylum1968No ratings yet
- Thesis Statement On Anabolic SteroidsDocument4 pagesThesis Statement On Anabolic SteroidsBuyThesisPaperVirginiaBeach100% (2)
- A Longitudinal Investigation of Sports-Related Risk Factors For Disordered Eating in Aesthetic SportsDocument8 pagesA Longitudinal Investigation of Sports-Related Risk Factors For Disordered Eating in Aesthetic Sportsfpetrelli_857303250No ratings yet
- Research On Anabolic SteroidsDocument6 pagesResearch On Anabolic SteroidsAnthony Sanglay, Jr.No ratings yet
- Anabolic Steroids Thesis StatementDocument6 pagesAnabolic Steroids Thesis StatementBestCollegePaperWritingServiceUK100% (2)
- Performance Enhancing Drugs in Baseball Research PaperDocument6 pagesPerformance Enhancing Drugs in Baseball Research Papertehajadof1k3No ratings yet
- Echocardiographic Findings in Power Athletes Abusing Anabolic Androgenic SteroidsDocument5 pagesEchocardiographic Findings in Power Athletes Abusing Anabolic Androgenic SteroidsSita PrasidaNo ratings yet
- Regular Aerobic Exercise Improves SexualDocument9 pagesRegular Aerobic Exercise Improves SexualAndresMoralesUrbinaNo ratings yet
- FinalDocument9 pagesFinaleatdickNo ratings yet
- Efeitos Da Deca em BodybuilDocument7 pagesEfeitos Da Deca em BodybuilPedro SilvaNo ratings yet
- Gls 078Document9 pagesGls 078GustNo ratings yet
- Steroids FactsDocument3 pagesSteroids Factsfaqed ilzakiraNo ratings yet
- (23915412 - Open Life Sciences) Anabolic Androgenic Steroids Effects On The Immune System A ReviewDocument15 pages(23915412 - Open Life Sciences) Anabolic Androgenic Steroids Effects On The Immune System A ReviewMiguel AngelNo ratings yet
- Riesgos Renales en El Uso de EAADocument12 pagesRiesgos Renales en El Uso de EAAsimon jaramilloNo ratings yet
- (14796805 - Journal of Endocrinology) Proof of The Effect of Testosterone On Skeletal MuscleDocument12 pages(14796805 - Journal of Endocrinology) Proof of The Effect of Testosterone On Skeletal MuscleDaveNo ratings yet
- Drug Use FinalDocument7 pagesDrug Use Finalapi-270008205No ratings yet
- Testosterone and Growth Hormone in Older Men For Better or For WorseDocument4 pagesTestosterone and Growth Hormone in Older Men For Better or For WorseGayathriMaranNo ratings yet
- Research Paper Steroids in SportsDocument8 pagesResearch Paper Steroids in Sportseffbd7j4100% (1)
- Research Paper SteroidsDocument4 pagesResearch Paper Steroidsgzzjhsv9100% (1)
- Dac 0808Document14 pagesDac 0808Jes SarGeNo ratings yet
- Irfr 9120 NPBFDocument11 pagesIrfr 9120 NPBFdsafhNo ratings yet
- HRPT 114 HR Fy2017 AgricultureDocument116 pagesHRPT 114 HR Fy2017 AgriculturedsafhNo ratings yet
- (Self-Help) A Mini Guide To Critical ThinkingDocument26 pages(Self-Help) A Mini Guide To Critical ThinkingchlscNo ratings yet
- Simple Modeling and Identification Procedures For " Black-Box " Behavioral Modeling of Power Converters Based On Transient Response Analysis - 2009Document15 pagesSimple Modeling and Identification Procedures For " Black-Box " Behavioral Modeling of Power Converters Based On Transient Response Analysis - 2009dsafhNo ratings yet
- (A) Small SIgnal Analysis of Energy Factor and MM For DC-DCDocument11 pages(A) Small SIgnal Analysis of Energy Factor and MM For DC-DCdsafhNo ratings yet
- (A) WANG, ModelingAnalysisAndApplicationOfBuckConvertersDocument11 pages(A) WANG, ModelingAnalysisAndApplicationOfBuckConvertersdsafhNo ratings yet
- Multiple AllelesDocument31 pagesMultiple AllelesJENNIFER DAVIDNo ratings yet
- c3 Molecular Genetics Unit PlanDocument20 pagesc3 Molecular Genetics Unit Planapi-477617112No ratings yet
- DNA Extraction and Polymerase Chain ReactionDocument2 pagesDNA Extraction and Polymerase Chain ReactionDudungNo ratings yet
- Integumentary System of VertebratesDocument4 pagesIntegumentary System of VertebratesJUANJOSEFOXNo ratings yet
- Name: Nhlakanipho Surname: Khwela Student No.: 61541524 Module Code: BLG1502 Assignment No.: 02 Unique Number: 711357Document8 pagesName: Nhlakanipho Surname: Khwela Student No.: 61541524 Module Code: BLG1502 Assignment No.: 02 Unique Number: 711357Nhlakana Kay KhwelaNo ratings yet
- Peter Duerre - Handbook On Clostridia-CRC Press (2004) PDFDocument1,156 pagesPeter Duerre - Handbook On Clostridia-CRC Press (2004) PDFaldea_844577109100% (1)
- General Biology 1 Workbook Pages 43 52Document12 pagesGeneral Biology 1 Workbook Pages 43 52R VHINo ratings yet
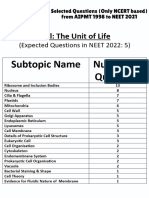
- Cell - The Unit of Life - NCERT Based PYQsDocument9 pagesCell - The Unit of Life - NCERT Based PYQsAkhil singhNo ratings yet
- Regulation of Endocrine System PhysiologyDocument169 pagesRegulation of Endocrine System PhysiologyCriss CristinaNo ratings yet
- RIZAL TECHNOLOGICAL UNIVERSITY Glossary of Key Environmental Engineering TermsDocument6 pagesRIZAL TECHNOLOGICAL UNIVERSITY Glossary of Key Environmental Engineering TermsMica GiananNo ratings yet
- Heredity and Variation.Document6 pagesHeredity and Variation.AnweNo ratings yet
- Animal BiotechnologyDocument50 pagesAnimal BiotechnologyJyotsna Ravikumar60% (10)
- Genetic diversity analysis of colored and white rice genotypes using Microsatellite (SSR) and Insertion-Deletion (INDEL) markersDocument11 pagesGenetic diversity analysis of colored and white rice genotypes using Microsatellite (SSR) and Insertion-Deletion (INDEL) markersMehvish ChNo ratings yet
- Cell Theory ACtivityDocument2 pagesCell Theory ACtivityMa.Janice Garcia0% (1)
- Jurnal: Identifikasi Kromosom Homolog Melalui Deteksi Pada Tanaman Bawang MerahDocument9 pagesJurnal: Identifikasi Kromosom Homolog Melalui Deteksi Pada Tanaman Bawang MerahImaniar FitriatasyaVWNo ratings yet
- SR5 TOOL Chrome Flesh IndexDocument2 pagesSR5 TOOL Chrome Flesh IndexBeki LokaNo ratings yet
- Willerman Et Al 91 Brain Size-IQDocument6 pagesWillerman Et Al 91 Brain Size-IQkaymmmmmmmNo ratings yet
- Nanobodies From Camelid Mice and Llamas Neutralize Sars-Cov-2 VariantsDocument26 pagesNanobodies From Camelid Mice and Llamas Neutralize Sars-Cov-2 VariantsCyril NoelNo ratings yet
- IJRPP - 14 - 303 Sai Priya MarrapuDocument4 pagesIJRPP - 14 - 303 Sai Priya MarrapuSamuel WilliamsNo ratings yet
- Bio150-80 Syllabus-Instructor Addendum-2016 Fall PDFDocument5 pagesBio150-80 Syllabus-Instructor Addendum-2016 Fall PDFFatmata BanguraNo ratings yet
- 1962, Waddington, How Animals DevelopDocument148 pages1962, Waddington, How Animals DevelopLuis Ossa FuentesNo ratings yet
- Placenta Extract & Castor Oil (Next Generation Wound Healer)Document11 pagesPlacenta Extract & Castor Oil (Next Generation Wound Healer)International Journal of Innovative Science and Research TechnologyNo ratings yet
- A Tool For The Analysis of Chromosomes: Karyotype: Taxon June 2016Document8 pagesA Tool For The Analysis of Chromosomes: Karyotype: Taxon June 2016Kelly Rios ZapataNo ratings yet
- How Living Things ReproduceDocument44 pagesHow Living Things ReproduceChristopher Agustin Tambogon LptNo ratings yet