You might also like
- 7sgdfgf PDFDocument438 pages7sgdfgf PDFPratik JadhavNo ratings yet
- Table of Genetic Disorders: Download A Copy of This Study GuideDocument11 pagesTable of Genetic Disorders: Download A Copy of This Study Guideerica perezNo ratings yet
- Table of Genetic DisordersDocument9 pagesTable of Genetic DisordersjeslymailNo ratings yet
- SketchyPath ChecklistDocument1 pageSketchyPath ChecklistGabriella RosinaNo ratings yet
- UW 2021 Notes - Lungs UsmleDocument422 pagesUW 2021 Notes - Lungs Usmlekathi raja sekhar100% (1)
- Heart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesDocument3 pagesHeart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesPrarthana Thiagarajan100% (3)
- Disease Pathognomonic Sign: Muddy Brown CastsDocument1 pageDisease Pathognomonic Sign: Muddy Brown CastsRafey AhmedNo ratings yet
- Pharmayield: Must Know Pharmacology NotesDocument2 pagesPharmayield: Must Know Pharmacology NotesBianca Desiree VergaraNo ratings yet
- SketchyPath ChecklistDocument1 pageSketchyPath ChecklistFajar Raza100% (1)
- Cocci Rod 4 Main Classifications: Gram Staph, Strep Bacillus Clostridium Neisseria Pleiomorphic Enterobact-EriceaeDocument2 pagesCocci Rod 4 Main Classifications: Gram Staph, Strep Bacillus Clostridium Neisseria Pleiomorphic Enterobact-EriceaeKimberly KanemitsuNo ratings yet
- Usmle Hy Step1Document20 pagesUsmle Hy Step1Sindu SaiNo ratings yet
- Hematology & Oncology. Anatomy 56Document60 pagesHematology & Oncology. Anatomy 56Heran TeferiNo ratings yet
- UW Infectious Diseases + Microbiology Educational Objectives PDFDocument75 pagesUW Infectious Diseases + Microbiology Educational Objectives PDFDrbee10No ratings yet
- Poliomyelitis Haemophilus Influenzae Type B VariecellaDocument4 pagesPoliomyelitis Haemophilus Influenzae Type B VariecellaJeanna Chong100% (1)
- Lippin NotesDocument8 pagesLippin Noteswalt65100% (1)
- Bipolar Disorder Background: Hypomania Has The Same Symptoms of Mania Without Psychotic SymptomsDocument2 pagesBipolar Disorder Background: Hypomania Has The Same Symptoms of Mania Without Psychotic SymptomshumdingerNo ratings yet
- Mental Health Activity ProposalDocument2 pagesMental Health Activity ProposalJustin Tagumasi Agustin100% (1)
- International Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessFrom EverandInternational Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessRaghav GovindarajanNo ratings yet
- UW (Step 1) Dermatology - Educational Objectives PDFDocument28 pagesUW (Step 1) Dermatology - Educational Objectives PDFUsama BilalNo ratings yet
- Large: Primary Adrenocortical Deficiency Pernicious AnemiaDocument28 pagesLarge: Primary Adrenocortical Deficiency Pernicious Anemiawaqasmumtaz12No ratings yet
- Complete Genetics Disease ChartDocument14 pagesComplete Genetics Disease ChartJames FlanneryNo ratings yet
- Pediatric Pathology: Disease Cause/Risk Factors SymptomsDocument12 pagesPediatric Pathology: Disease Cause/Risk Factors SymptomsherethemindNo ratings yet
- Actinic KeratosisDocument19 pagesActinic Keratosisattydoc1234No ratings yet
- Clinical Algorithms in General Surgery PDFDocument786 pagesClinical Algorithms in General Surgery PDFLaura Campaña100% (5)
- USMLE NotesDocument165 pagesUSMLE NotesHerliani HalimNo ratings yet
- Flash Notes SyndromesDocument8 pagesFlash Notes SyndromesschxzerrydawnNo ratings yet
- Internal Medicine NBME Form 3 ExplanationsDocument11 pagesInternal Medicine NBME Form 3 ExplanationssasghfdgNo ratings yet
- UW (Step 1) Biochemistry - Educational ObjectivesDocument41 pagesUW (Step 1) Biochemistry - Educational ObjectivesUsama BilalNo ratings yet
- Renal - PathDocument23 pagesRenal - PathKimberly KanemitsuNo ratings yet
- Zanki (Complete) + R/medicalschoolanki Microbiology ErrataDocument70 pagesZanki (Complete) + R/medicalschoolanki Microbiology ErrataedNo ratings yet
- VW Golf 8 Variant WD EngDocument664 pagesVW Golf 8 Variant WD EngLakhdar BouchenakNo ratings yet
- DRTPAnnouncementEN PDFDocument1 pageDRTPAnnouncementEN PDFSinaShafaatiNo ratings yet
- L-6th Sem (Eng Notes) Law Relating To Women and ChildDocument52 pagesL-6th Sem (Eng Notes) Law Relating To Women and ChildCuriae corporate consultantsNo ratings yet
- Anatomy Shelf Notes Dw9Document200 pagesAnatomy Shelf Notes Dw9Zain ul abedinNo ratings yet
- Ahmed Samir - Step 1 Experience - 251Document16 pagesAhmed Samir - Step 1 Experience - 251Mohamed LoaiNo ratings yet
- Automobile Air Conditioning SystemDocument8 pagesAutomobile Air Conditioning SystemAyyan Gaonkhadkar100% (1)
- Leonard Peikoff-Introduction To LogicDocument20 pagesLeonard Peikoff-Introduction To Logicbursa07No ratings yet
- Hookah Bar Business PlanDocument34 pagesHookah Bar Business PlanAbdelkebir LabyadNo ratings yet
- Vertical Mills V2 0Document56 pagesVertical Mills V2 0recai100% (1)
- Exam 1 DiseasesDocument1 pageExam 1 DiseasesSolomon Seth SallforsNo ratings yet
- Anti FungalsDocument5 pagesAnti FungalskakuNo ratings yet
- Ebr Hy CluesDocument16 pagesEbr Hy CluesStaporn KasemsripitakNo ratings yet
- 2-Month Usmle Step 1 Sample ScheduleDocument4 pages2-Month Usmle Step 1 Sample ScheduleSuggula Vamsi KrishnaNo ratings yet
- Diseases - BiochemDocument4 pagesDiseases - BiochemJay FeldmanNo ratings yet
- Brenner and Stevens, Pharmacology 3 © 2010Document5 pagesBrenner and Stevens, Pharmacology 3 © 2010PharAwayNo ratings yet
- Mnemonics Step 1Document4 pagesMnemonics Step 1Raji NaamaniNo ratings yet
- Anemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDocument15 pagesAnemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDanielle FosterNo ratings yet
- Bio Chem 1Document5 pagesBio Chem 1Reynaldo RiveraNo ratings yet
- Path DumpsDocument44 pagesPath DumpsAndleeb ImranNo ratings yet
- COMBANK Level 1 2019Document16 pagesCOMBANK Level 1 2019aloverofdance0% (1)
- First Aid PharmacoDocument61 pagesFirst Aid PharmacogirNo ratings yet
- Renal SystemDocument76 pagesRenal SystemDaNy ChiriacNo ratings yet
- Workbook of BiochemDocument22 pagesWorkbook of BiochemMedStudent MedStudentNo ratings yet
- Microbiology (Notes From Uworld)Document2 pagesMicrobiology (Notes From Uworld)Nanda MinndinNo ratings yet
- Arya. Skin Path LabDocument54 pagesArya. Skin Path LabMJO79No ratings yet
- 4.1d - Pathology of The Pituitary - Nov.10 - Dr. GalangDocument4 pages4.1d - Pathology of The Pituitary - Nov.10 - Dr. GalangMiel Raphael AranillaNo ratings yet
- Repro Costanzo NotesDocument11 pagesRepro Costanzo NotesAbeebs SalahouNo ratings yet
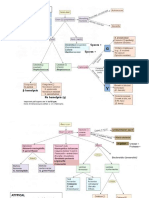
- Retinoblastoma Cognitive Concept Map - DR Kumar Ponnusamy and DR Jegathambigai RN - Problem Based Learning (PBL) For Large Groups Medical StudentsDocument1 pageRetinoblastoma Cognitive Concept Map - DR Kumar Ponnusamy and DR Jegathambigai RN - Problem Based Learning (PBL) For Large Groups Medical StudentsPonnusamy Kumar100% (1)
- Patho Common Stuff - RobbinsDocument7 pagesPatho Common Stuff - RobbinsMaf BNo ratings yet
- Genetic Disorders-Www - Qworld.co - inDocument13 pagesGenetic Disorders-Www - Qworld.co - inQworld100% (1)
- SketchyMicro ChartDocument8 pagesSketchyMicro ChartAnna A.No ratings yet
- Behavioral FinalsDocument28 pagesBehavioral FinalsKofiBNo ratings yet
- QuizletDocument104 pagesQuizletS.No ratings yet
- Malassezia Furfur An-An Ap-Ap Naturally Found On The SkinDocument48 pagesMalassezia Furfur An-An Ap-Ap Naturally Found On The SkinNikki ValerioNo ratings yet
- Pathology Description/Buzz Words DiseaseDocument5 pagesPathology Description/Buzz Words Diseasebea manzanoNo ratings yet
- Exp 4 Centrifugal CompressorDocument11 pagesExp 4 Centrifugal CompressorFaris HamirNo ratings yet
- Winchester Model 9422 Lever Action Rifle Owner's Manual: LicenseeDocument0 pagesWinchester Model 9422 Lever Action Rifle Owner's Manual: Licenseecarlosfanjul1No ratings yet
- Daily 500 Maximum 2500 Minimum 1000 Lead Time 15 Days EOQ 1200 Emergency Lead Time 3 DaysDocument5 pagesDaily 500 Maximum 2500 Minimum 1000 Lead Time 15 Days EOQ 1200 Emergency Lead Time 3 DaysM Noaman AkbarNo ratings yet
- World Wide Emission Free E-Motercycle ProjectDocument20 pagesWorld Wide Emission Free E-Motercycle ProjectAkshay SharmaNo ratings yet
- Geotechnical Engineering GATE Previous QuestionsDocument35 pagesGeotechnical Engineering GATE Previous QuestionsSurya ChejerlaNo ratings yet
- Leader Ship Assessment: Student No 374212036Document4 pagesLeader Ship Assessment: Student No 374212036Emily KimNo ratings yet
- AcuityPDR BrochureDocument3 pagesAcuityPDR BrochureJulian HutabaratNo ratings yet
- Yuasa NPL Range: VRLA BatteriesDocument2 pagesYuasa NPL Range: VRLA BatteriesVuro BegaNo ratings yet
- Juri Ferrer - Ws - WeatherDocument4 pagesJuri Ferrer - Ws - WeathersJIqsNo ratings yet
- Catalog en Eurocoustic 0Document132 pagesCatalog en Eurocoustic 0Vikash KumarNo ratings yet
- Exam G-9 CookeryDocument5 pagesExam G-9 Cookeryaileenarcabal01No ratings yet
- CombinedList PDFDocument3 pagesCombinedList PDFMarie BautistaNo ratings yet
- Bellows and Expansion JointsDocument5 pagesBellows and Expansion JointsSuresh MechNo ratings yet
- Most Important Electrical Engineering NTS Based Short QuestionsDocument63 pagesMost Important Electrical Engineering NTS Based Short QuestionsnageenNo ratings yet
- Excel HysysDocument11 pagesExcel HysysAndrie Kurniawan IndraNo ratings yet
- Parenting Styles and Social Interaction of Senior Secondary School Students in Imo State, NigeriaDocument10 pagesParenting Styles and Social Interaction of Senior Secondary School Students in Imo State, NigeriaInternational Educational Applied Scientific Research Journal (IEASRJ)No ratings yet
- Endovascular Skills CourseDocument20 pagesEndovascular Skills CourseAbdullah JibawiNo ratings yet
- POFL Unit 1 Status QUO pp.1-37Document38 pagesPOFL Unit 1 Status QUO pp.1-37AruNo ratings yet
- UNIT-5 International Dimensions To Industrial Relations: ObjectivesDocument27 pagesUNIT-5 International Dimensions To Industrial Relations: ObjectivesManish DwivediNo ratings yet
- What Is A Walkable Place The Walkability Debate inDocument20 pagesWhat Is A Walkable Place The Walkability Debate inBADR HAMDAN ALATEBENo ratings yet
- Preparation of Stick Type Solid Glue As Paper AdheDocument9 pagesPreparation of Stick Type Solid Glue As Paper AdheAhmad AlShahrourNo ratings yet
- 2013 Medigate Profile PDFDocument26 pages2013 Medigate Profile PDFGabriel Duran DiazNo ratings yet