You might also like
- 32476C/P3 Work Placement Portfolio: 1. Background/overviewDocument31 pages32476C/P3 Work Placement Portfolio: 1. Background/overviewtetyanaNo ratings yet
- High Blood Pressure: Safe alternatives without drugsFrom EverandHigh Blood Pressure: Safe alternatives without drugsRating: 5 out of 5 stars5/5 (2)
- Nursing Care Plan Knowledge DeficientDocument1 pageNursing Care Plan Knowledge Deficientderic100% (11)
- Carranza 12e - Furcation Involvement and TreatmentDocument14 pagesCarranza 12e - Furcation Involvement and TreatmentK KNo ratings yet
- Strain Counter-Strain PDFDocument7 pagesStrain Counter-Strain PDFCarlosCarpinteroRubioNo ratings yet
- Blood PressureDocument18 pagesBlood PressureManar Magdy100% (1)
- Postural Vital Signs MeasurementRevisedDocument8 pagesPostural Vital Signs MeasurementRevisedumiNo ratings yet
- BP - LippincottDocument7 pagesBP - LippincottForrest LloydNo ratings yet
- NCM Checklist - Vital SignsDocument18 pagesNCM Checklist - Vital SignsYanna Habib-Mangotara100% (1)
- Tension Arterial..Trabajo en InglesDocument4 pagesTension Arterial..Trabajo en InglesMari Alvarado BravoNo ratings yet
- Assessing Blood PressureDocument14 pagesAssessing Blood PressureMrs RehanNo ratings yet
- Measuring Vital Signs: How To Take Blood PressureDocument5 pagesMeasuring Vital Signs: How To Take Blood PressureErin BarnesNo ratings yet
- Assessing Blood PressureDocument4 pagesAssessing Blood PressureCraigyyNo ratings yet
- Taking Blood Pressure ManuallyDocument2 pagesTaking Blood Pressure ManuallyManoj Kumar GNo ratings yet
- WECOC - Diagnosing HypertensionDocument37 pagesWECOC - Diagnosing HypertensionDhira 'Princess Kalonk' AninditaNo ratings yet
- Postural HypotensionDocument3 pagesPostural HypotensionSimran JosanNo ratings yet
- Assessing Vital Signs: Blood Pressure: Myra E. Sosas, RN, ManDocument27 pagesAssessing Vital Signs: Blood Pressure: Myra E. Sosas, RN, ManMyra E. SosasNo ratings yet
- BloodpressureDocument4 pagesBloodpressureLiana Koh VillanuevaNo ratings yet
- Demonstration On BPDocument7 pagesDemonstration On BPpritidinda3070No ratings yet
- Blood PressureDocument9 pagesBlood Pressuregenevieve kryzleiNo ratings yet
- Vital Signs Taking: Ms. Kristine Uy-Urgena, RN, MN College of Nursing Xavier University - Ateneo de Cagayan NCM 101 RleDocument19 pagesVital Signs Taking: Ms. Kristine Uy-Urgena, RN, MN College of Nursing Xavier University - Ateneo de Cagayan NCM 101 RleJanieza BaltazarNo ratings yet
- Taking Blood Pressure CorrectlyDocument7 pagesTaking Blood Pressure CorrectlySamue100% (1)
- Data About HPNDocument24 pagesData About HPNAdrhien Ciane ManzanoNo ratings yet
- Measuring Vital Signs: How To Take Blood PressureDocument5 pagesMeasuring Vital Signs: How To Take Blood PressureErin BarnesNo ratings yet
- M.Heldi Riyanda 19334059 B InggrisDocument3 pagesM.Heldi Riyanda 19334059 B InggrisBintan NajihanNo ratings yet
- Procedure in Assessing Blood PressureDocument4 pagesProcedure in Assessing Blood PressurecrrfrncNo ratings yet
- Taking The Vital SignsDocument6 pagesTaking The Vital SignsAaron RoxasNo ratings yet
- Assessing Blood PressureDocument3 pagesAssessing Blood PressureSean DuayNo ratings yet
- Assessing A Brachial Artery Blood PressureDocument21 pagesAssessing A Brachial Artery Blood PressureEric ParmleyNo ratings yet
- DR Tarun BhatnagarDocument40 pagesDR Tarun Bhatnagararhim aljalyNo ratings yet
- Vital Signs Examination - Kuliah SMT 2 2008Document54 pagesVital Signs Examination - Kuliah SMT 2 2008VilasineeAriHaraKumarNo ratings yet
- Directions For Use of An Aneroid Sphygmomanometer PDFDocument6 pagesDirections For Use of An Aneroid Sphygmomanometer PDFNana AkwaboahNo ratings yet
- Taking Blood PressureDocument3 pagesTaking Blood PressureApril Iren Claire BalabalaNo ratings yet
- Limba Engleza: Universitatea Bioterra Bucuresti Facultatea de Asistenta Medicala GeneralaDocument3 pagesLimba Engleza: Universitatea Bioterra Bucuresti Facultatea de Asistenta Medicala GeneralaCristina CrisuNo ratings yet
- Classification of Overweight and Obesity by Bmi: A. BP Automated Ambulatory Blood Pressure Monitoring MeasuresDocument8 pagesClassification of Overweight and Obesity by Bmi: A. BP Automated Ambulatory Blood Pressure Monitoring MeasuresemmanuelNo ratings yet
- Pengukuran Tekanan Darah Dan NadiDocument22 pagesPengukuran Tekanan Darah Dan NadiBellaNo ratings yet
- BP ChecklistDocument4 pagesBP Checklistkuroko senpaiNo ratings yet
- Unit 05 Admitting Patients: Reading 02 Taking Blood Pressure ManuallyDocument3 pagesUnit 05 Admitting Patients: Reading 02 Taking Blood Pressure Manuallyila syadiahNo ratings yet
- Vital SignDocument100 pagesVital SignIbnu FuqonNo ratings yet
- Surgical Ho Guide1Document35 pagesSurgical Ho Guide1puravi91No ratings yet
- Practical Nursing Diploma Program Nursing Skills Lab 1: Blood Pressure Week 12Document21 pagesPractical Nursing Diploma Program Nursing Skills Lab 1: Blood Pressure Week 12Taryn CorbettNo ratings yet
- Blood Pressure 01Document23 pagesBlood Pressure 01Fahad MahmoodNo ratings yet
- MAKALAH BHS INGGRIS BLOOD PRESSURE BruDocument8 pagesMAKALAH BHS INGGRIS BLOOD PRESSURE Brudik rushcompNo ratings yet
- Lesson-7 Blood Pressure 2019-2020-24709Document43 pagesLesson-7 Blood Pressure 2019-2020-24709Maria OnofrașNo ratings yet
- Blood Pressure MeasurementDocument1 pageBlood Pressure Measurementapi-76740522No ratings yet
- Clinical HypertensionDocument18 pagesClinical Hypertensionsatyajeev soburrunNo ratings yet
- Blood Pressure NoteDocument2 pagesBlood Pressure NoteShahnaz DarNo ratings yet
- Blood PressureDocument4 pagesBlood PressureWincy SalazarNo ratings yet
- S Phy Gmo ManometerDocument16 pagesS Phy Gmo ManometerNana AkwaboahNo ratings yet
- Blood Pressure MeasurementDocument24 pagesBlood Pressure MeasurementCahyi MardiantiNo ratings yet
- Fakultas Kedokteran UnisbaDocument28 pagesFakultas Kedokteran UnisbadeasyahNo ratings yet
- How To Check BPDocument1 pageHow To Check BPFAZARA SabilaAlzNo ratings yet
- Aubrey Rose A. Vidon BSN 3Y1-2 Course Unit #1Document3 pagesAubrey Rose A. Vidon BSN 3Y1-2 Course Unit #1AriaNo ratings yet
- Blood Pressure MeasurementDocument2 pagesBlood Pressure MeasurementMaryHope100% (1)
- UNIT 7 Vital Signs BPDocument22 pagesUNIT 7 Vital Signs BPsaranya amuNo ratings yet
- Bloodpressure 2Document4 pagesBloodpressure 2Yousuf Azhar AlamiaNo ratings yet
- Physiology 3Document28 pagesPhysiology 3Chuan RuiNo ratings yet
- Measurement of BPDocument6 pagesMeasurement of BPNiko DagunoNo ratings yet
- Ateneo de Zamboanga UniversityDocument5 pagesAteneo de Zamboanga UniversityLizzey YuNo ratings yet
- Vital Signs/'Document30 pagesVital Signs/'Monika MinhasNo ratings yet
- 7 Assessing Blood PressureDocument5 pages7 Assessing Blood PressureMarky RoqueNo ratings yet
- Blood Pressure Practical Dec 2020Document27 pagesBlood Pressure Practical Dec 2020bvkjtzrvnyNo ratings yet
- Arteri LineDocument13 pagesArteri Linemuthia octavianaNo ratings yet
- Blood Pressure: Step By Step Guide And Proven Recipes To Lower Your Blood Pressure Without Any MedicationFrom EverandBlood Pressure: Step By Step Guide And Proven Recipes To Lower Your Blood Pressure Without Any MedicationNo ratings yet
- Community Organizing Participatory Research (COPAR)Document4 pagesCommunity Organizing Participatory Research (COPAR)mArLoN91% (11)
- Community Organizing Participatory Research (COPAR)Document4 pagesCommunity Organizing Participatory Research (COPAR)mArLoN91% (11)
- Signs of Illness and InjuryDocument2 pagesSigns of Illness and InjurywyndzNo ratings yet
- Types & Causes of Open WoundsDocument3 pagesTypes & Causes of Open WoundsmArLoNNo ratings yet
- Therapeutic DietsDocument8 pagesTherapeutic DietsmArLoN91% (11)
- Herbal Medicines Plants Approved by The DOHDocument3 pagesHerbal Medicines Plants Approved by The DOHmArLoN100% (2)
- Dosage CalculationsDocument39 pagesDosage Calculationssalak9462900% (1)
- PremedicationDocument9 pagesPremedicationdrhiwaomer100% (3)
- Clavien Dildo Complications Assesment in Bariatric SurgeryDocument6 pagesClavien Dildo Complications Assesment in Bariatric SurgeryErlan SantosNo ratings yet
- The Effectiveness of Hypnotherapy in Reducing PainDocument7 pagesThe Effectiveness of Hypnotherapy in Reducing PainArie DwianggaNo ratings yet
- Learning: Concepts, Principles and Nature!Document15 pagesLearning: Concepts, Principles and Nature!amrendrakr090% (1)
- Drug StudyDocument6 pagesDrug StudyIrveen Joy RamirezNo ratings yet
- Training Individuals With Mental Retardation For Independent Living - Social Skills - Understanding OneselfDocument17 pagesTraining Individuals With Mental Retardation For Independent Living - Social Skills - Understanding OneselfMicah Camille CaramatNo ratings yet
- Loss, Grief and End-of-Life CareDocument30 pagesLoss, Grief and End-of-Life CareMarwa AliNo ratings yet
- Of Class Has: Kinanthropometry in Aquatic Sports: A Study World AthletesDocument1 pageOf Class Has: Kinanthropometry in Aquatic Sports: A Study World AthletesBrayam AguilarNo ratings yet
- Best Practice For Occupation Focused PracticeDocument18 pagesBest Practice For Occupation Focused PracticeKrista HoerstenNo ratings yet
- Acute Respiratory Distress in ChildrenDocument25 pagesAcute Respiratory Distress in Childrensai ram100% (1)
- Guidline Threatment For of Alcohol Use DisorderDocument226 pagesGuidline Threatment For of Alcohol Use Disorderafifberlian100% (1)
- Arylcyclohexamines (Ketamine, Phencyclidine, and Analogues)Document47 pagesArylcyclohexamines (Ketamine, Phencyclidine, and Analogues)gigidurul1111100% (1)
- Test Bank Chapter 5: Psychosocial Alterations: Urden: Thelan's Critical Care Nursing, 5 EditionDocument8 pagesTest Bank Chapter 5: Psychosocial Alterations: Urden: Thelan's Critical Care Nursing, 5 EditionAnonymous ZzjzIcmNo ratings yet
- Rehabilitation of Sports Injuries - Scientific BasisDocument338 pagesRehabilitation of Sports Injuries - Scientific Basisjimitkapadia100% (3)
- Comparative Efficacy of Non-Sedating Antihistamine Updosing in Patients With Chronic UrticariaDocument6 pagesComparative Efficacy of Non-Sedating Antihistamine Updosing in Patients With Chronic UrticariadregleavNo ratings yet
- Anesthesia For Cesarean SectionDocument84 pagesAnesthesia For Cesarean SectionssamaddNo ratings yet
- Acute GastritisDocument14 pagesAcute GastritisMenchie Vivas-AlotNo ratings yet
- Guidelines For High Flow Oxygen Therapy (AIRVO ) On The WardsDocument11 pagesGuidelines For High Flow Oxygen Therapy (AIRVO ) On The WardsBurhanNo ratings yet
- Right Sided Heart Failure Case 4.2Document4 pagesRight Sided Heart Failure Case 4.2Athari AdityaNo ratings yet
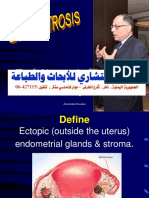
- Endometriosis 140727182255 Phpapp01Document182 pagesEndometriosis 140727182255 Phpapp01bmhsh100% (1)
- Glomus TumorDocument14 pagesGlomus Tumorhardrocker_2007No ratings yet
- Case of Febrile SeizuresDocument2 pagesCase of Febrile SeizuresAzizan HannyNo ratings yet
- An Interview With Henny HeudensDocument7 pagesAn Interview With Henny HeudensDr Dushyant Kamal Dhari100% (1)
- Acute Respiratory Distress SyndromeDocument30 pagesAcute Respiratory Distress SyndromeNikhil GhubadeNo ratings yet
- Problem Statement: "Effectiveness of Mint Leaves Paste On Dysmenorrhea Among Adolescent Girls"Document12 pagesProblem Statement: "Effectiveness of Mint Leaves Paste On Dysmenorrhea Among Adolescent Girls"tanmai nooluNo ratings yet
- Cancer and Pregnancy PDFDocument254 pagesCancer and Pregnancy PDFAdina MeregiuNo ratings yet