You might also like
- What Is The Oxygen CascadeDocument27 pagesWhat Is The Oxygen CascadeRandhir Singh90% (10)
- Transport of Oxygen and Carbon Dioxide-PartialDocument24 pagesTransport of Oxygen and Carbon Dioxide-PartialMarie PetalcorinNo ratings yet
- How Gases Are Transported in the BloodDocument22 pagesHow Gases Are Transported in the BloodAiza AyazNo ratings yet
- Chapter 5 Cell RespirationDocument12 pagesChapter 5 Cell Respirationaznknight323No ratings yet
- Regulation of Oxidative PhosphorylationDocument14 pagesRegulation of Oxidative Phosphorylationmaaz629No ratings yet
- Biochemistry: Elizabeth's Step 1 Power ReviewDocument67 pagesBiochemistry: Elizabeth's Step 1 Power ReviewMikey PalominoNo ratings yet
- Nutrition and Cancer Salvestrol Case Studies Schaefer2007Document6 pagesNutrition and Cancer Salvestrol Case Studies Schaefer2007Matthew MabryNo ratings yet
- Carnitine Deficiency: Structure, Function, Metabolism and DeficiencyDocument58 pagesCarnitine Deficiency: Structure, Function, Metabolism and DeficiencyRafael Francisco Garcia Munoz100% (1)
- Beta OxidationDocument25 pagesBeta OxidationManoj SigdelNo ratings yet
- Phytoalexins PhytoanticipinsDocument3 pagesPhytoalexins PhytoanticipinsSébastien BellowNo ratings yet
- Biochemistry 1.01 Cell MembraneDocument8 pagesBiochemistry 1.01 Cell MembraneApril AramNo ratings yet
- 02 HemoglobinDocument78 pages02 HemoglobinpixiedustNo ratings yet
- HomeostasisDocument35 pagesHomeostasisPranshu AdityaNo ratings yet
- Oxidation in Fats & Oils by P-Anisidine ValueDocument2 pagesOxidation in Fats & Oils by P-Anisidine ValueAJNo ratings yet
- Fatty Acid OxidationDocument28 pagesFatty Acid OxidationEmm NomanNo ratings yet
- Ketosis & KetoacidosisDocument23 pagesKetosis & KetoacidosisrohishaakNo ratings yet
- ANICIDINEDocument14 pagesANICIDINEnityaNo ratings yet
- Oxygen Transport: Dr. Phoebe Bacalso-LetabaDocument36 pagesOxygen Transport: Dr. Phoebe Bacalso-LetabaMaria Nicole EconasNo ratings yet
- Structure of Myoglobin-RevDocument33 pagesStructure of Myoglobin-Revesubalew diressNo ratings yet
- Heme Synthesis Breakdown HBDocument18 pagesHeme Synthesis Breakdown HBDr.P.NatarajanNo ratings yet
- CH 6 Cellular RespirationDocument28 pagesCH 6 Cellular RespirationANo ratings yet
- Understanding Omega Fatty AcidsDocument5 pagesUnderstanding Omega Fatty Acidsdrubwang100% (1)
- Amino Acids Metabol Synth of UreaDocument32 pagesAmino Acids Metabol Synth of UreaAnastasiafynn100% (1)
- Iron's Role in Hemoglobin and Myoglobin CyclesDocument45 pagesIron's Role in Hemoglobin and Myoglobin CyclesnajwaNo ratings yet
- Hydrazine CancerDocument12 pagesHydrazine CancerAnonymous yL790SIeHNo ratings yet
- Cellular Respiration: MitochondriaDocument8 pagesCellular Respiration: MitochondriaMaryRoseTrajada100% (1)
- Metabolism of HemoglobinDocument46 pagesMetabolism of Hemoglobinlayla hitaNo ratings yet
- HaemoglobinDocument55 pagesHaemoglobinPhysiology by Dr RaghuveerNo ratings yet
- Oxidative Stress - Molecular Mechanisms and Biological EffectsDocument374 pagesOxidative Stress - Molecular Mechanisms and Biological EffectsEML100% (2)
- Mitochondria and Its Pathways: Arvin G. Concha Mst-BioDocument17 pagesMitochondria and Its Pathways: Arvin G. Concha Mst-Biocassidy conchaNo ratings yet
- 6.1 Types of NutritionDocument11 pages6.1 Types of NutritionNoor Hidayah SambliNo ratings yet
- Kreb CycleDocument6 pagesKreb Cycle211BT014 Jeev Sheen JosephNo ratings yet
- Xenobiotic MetabolismDocument64 pagesXenobiotic MetabolismBelajar dan berdoaNo ratings yet
- Maintaining Internal BalanceDocument6 pagesMaintaining Internal BalanceJayrelle D. SafranNo ratings yet
- Oxidative StressDocument53 pagesOxidative Stressapi-3723327100% (2)
- Transport of OxygenDocument13 pagesTransport of OxygenSiti Nurkhaulah JamaluddinNo ratings yet
- Myoglobin & Hemoglobin MyoglobinDocument8 pagesMyoglobin & Hemoglobin MyoglobinRajashree BoseNo ratings yet
- Carbohydrate ChemistryDocument2 pagesCarbohydrate ChemistryLakshmi VenkataramanNo ratings yet
- M.Prasad Naidu MSC Medical Biochemistry, Ph.D.Research ScholarDocument17 pagesM.Prasad Naidu MSC Medical Biochemistry, Ph.D.Research ScholarDr. M. Prasad Naidu100% (1)
- How Cells Harvest Chemical Energy - Cellular RespirationDocument25 pagesHow Cells Harvest Chemical Energy - Cellular RespirationMohamad Saadatian SipanNo ratings yet
- Alstonine, Flavopereirine, Sempervirine, Serpentine, Pao Pereira, RauwolfiaDocument9 pagesAlstonine, Flavopereirine, Sempervirine, Serpentine, Pao Pereira, RauwolfiaLeonardo NgoveneNo ratings yet
- Hydrogen Bonds & Solubility in WaterDocument8 pagesHydrogen Bonds & Solubility in WaternaifNo ratings yet
- Beta OxidationDocument29 pagesBeta Oxidationprism1702No ratings yet
- Biochemistry of Kidneys and UrineDocument18 pagesBiochemistry of Kidneys and UrineAndrias PutriNo ratings yet
- Cholesterol and Lipoprotein MetabolismDocument32 pagesCholesterol and Lipoprotein MetabolismBenjamin PrabhuNo ratings yet
- Understanding The Warburg Effect - The Metabolic Requirements of Cell ProliferationDocument12 pagesUnderstanding The Warburg Effect - The Metabolic Requirements of Cell Proliferationbowai741No ratings yet
- Gas TransportDocument10 pagesGas TransportDaveNo ratings yet
- Aerobic & Anaerobic Respiration: Biology Form 4Document36 pagesAerobic & Anaerobic Respiration: Biology Form 4Natalia SandyNo ratings yet
- Lecture 1 - Gene Transfer in BacteriaDocument52 pagesLecture 1 - Gene Transfer in BacteriaAbraham Kang0% (1)
- Purine Metabolism de Novo Synthesis and Salvage Pathway, 2015Document28 pagesPurine Metabolism de Novo Synthesis and Salvage Pathway, 2015Tehreem NadeemNo ratings yet
- Hormonal RegulationDocument5 pagesHormonal RegulationraizizaNo ratings yet
- Preventing and Reversing Cancer - The Absolute Health Integrative Oncology MethodDocument56 pagesPreventing and Reversing Cancer - The Absolute Health Integrative Oncology MethodHalal Media MalaysiaNo ratings yet
- Beta-Oxidation of Fatty AcidsDocument6 pagesBeta-Oxidation of Fatty AcidsBinku Dutta100% (1)
- Reference Ranges For Blood TestsDocument38 pagesReference Ranges For Blood TestscatalinNo ratings yet
- 1 Red Blood Cells Anemia and PolycythemiaDocument43 pages1 Red Blood Cells Anemia and PolycythemiaGeevee Naganag VentulaNo ratings yet
- Complex Ions ExplainedDocument5 pagesComplex Ions ExplainedRendy Ahmad LubisNo ratings yet
- 16.eating DisorderDocument17 pages16.eating DisorderSyahmi IeskandarNo ratings yet
- GTU 201 Kesihatan Dan Masyarakat Dr. Rohani Ismail Pusat Pengajian Sains KesihatanDocument13 pagesGTU 201 Kesihatan Dan Masyarakat Dr. Rohani Ismail Pusat Pengajian Sains KesihatanSyahmi IeskandarNo ratings yet
- Transport of Respiratory GasesDocument27 pagesTransport of Respiratory GasesSyahmi Ieskandar100% (1)
- Anatomy of Digestive Sys Large IntestineDocument60 pagesAnatomy of Digestive Sys Large IntestineSyahmi IeskandarNo ratings yet
- Basic EpidemiologyDocument226 pagesBasic EpidemiologyvladimirjazzNo ratings yet
- Regulation of Food IntakeDocument17 pagesRegulation of Food IntakeSyahmi IeskandarNo ratings yet
- Principle of Nutrition (GTN207) Dietary Reference Intakes: By: Dr. Hamid Jan B. Jan MohamedDocument15 pagesPrinciple of Nutrition (GTN207) Dietary Reference Intakes: By: Dr. Hamid Jan B. Jan MohamedSyahmi IeskandarNo ratings yet
- Anatomy of The Pharynx and Esophagus 2012Document44 pagesAnatomy of The Pharynx and Esophagus 2012Syahmi IeskandarNo ratings yet
- Mouth-Tongue Teeth-Esop Dec 2011-2012 SEM II - Prof FaridDocument51 pagesMouth-Tongue Teeth-Esop Dec 2011-2012 SEM II - Prof FaridSyahmi IeskandarNo ratings yet
- IntroductionDocument19 pagesIntroductionSyahmi IeskandarNo ratings yet
- Anatomy of Digestive Sys Stomach&Si 2012Document67 pagesAnatomy of Digestive Sys Stomach&Si 2012Syahmi IeskandarNo ratings yet
- Fluid Challenge RevisitedDocument5 pagesFluid Challenge RevisitedFernando Pinto AlvarezNo ratings yet
- Medical Emergencies in OSDocument62 pagesMedical Emergencies in OSAditi RapriyaNo ratings yet
- PROGRAMME ABSTRACT BOOK IACS ES 4 7 Oct 2023 Timisoara Romania - CORRDocument164 pagesPROGRAMME ABSTRACT BOOK IACS ES 4 7 Oct 2023 Timisoara Romania - CORRAlex MircescuNo ratings yet
- Peripheral Vascular DiseaseDocument32 pagesPeripheral Vascular DiseaseShy PatelNo ratings yet
- AQA A2 Biology Revision NotesDocument46 pagesAQA A2 Biology Revision NotesShiv SongaraNo ratings yet
- 18-93 Mini Project Final ReportDocument26 pages18-93 Mini Project Final ReportKP REDDYNo ratings yet
- PG BOTANY Plant Physiology Question Bank CompleteDocument10 pagesPG BOTANY Plant Physiology Question Bank CompleteAbid ShowketNo ratings yet
- Document 30Document7 pagesDocument 30SNIGDHA PATLOLANo ratings yet
- DSE Biology Chapter 3A - Essential life processes in plants 植物維持生命的活動Document24 pagesDSE Biology Chapter 3A - Essential life processes in plants 植物維持生命的活動liNo ratings yet
- A Typical ECG Tracing of The Cardiac CycleDocument3 pagesA Typical ECG Tracing of The Cardiac CycleMhiyciel UyNo ratings yet
- High-Intensity Interval Training, Solutions To The Programming Puzzle: Part I: Cardiopulmonary EmphasisDocument29 pagesHigh-Intensity Interval Training, Solutions To The Programming Puzzle: Part I: Cardiopulmonary EmphasisОстојић СтрахињаNo ratings yet
- ECG EquinoDocument19 pagesECG EquinoAgro PetNo ratings yet
- PhysioEx Exercise 10 Activity 4Document3 pagesPhysioEx Exercise 10 Activity 4Isabel PalaciosNo ratings yet
- Structure and Function of HaemoglobinDocument21 pagesStructure and Function of HaemoglobinEmily HoNo ratings yet
- Cell Signaling: Distant Location Near by CellsDocument20 pagesCell Signaling: Distant Location Near by CellsZEE zeeNo ratings yet
- 2020 ECC GuidelinesDocument32 pages2020 ECC GuidelinesKevin Michael Reyes Roque100% (1)
- 6 DefibrillationDocument22 pages6 DefibrillationrohithNo ratings yet
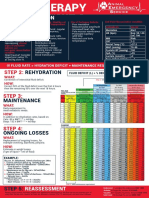
- FLUIDTHERAPY STEP 1: PERFUSIONDocument1 pageFLUIDTHERAPY STEP 1: PERFUSIONChristian De Leon100% (1)
- Cardiovascular Physiology Case StudiesDocument5 pagesCardiovascular Physiology Case StudiesAdie94No ratings yet
- Endocrine System & Major Organs (1-4)Document6 pagesEndocrine System & Major Organs (1-4)april lou andrea sorillaNo ratings yet
- Power Breathing Breathe Your Way To Inner Power (2008)Document260 pagesPower Breathing Breathe Your Way To Inner Power (2008)Prashant Patil100% (2)
- Neurostimulation For Stroke RehabilitationDocument11 pagesNeurostimulation For Stroke Rehabilitationisos.mporei.vevaios.No ratings yet
- Biology worksheet answersDocument2 pagesBiology worksheet answersAziyaNo ratings yet
- Unlock-Forensik Etik Medikolegal - PESERTADocument156 pagesUnlock-Forensik Etik Medikolegal - PESERTAAde fathNo ratings yet
- Angina PectorisDocument7 pagesAngina PectorisMovie Clips InternationalNo ratings yet
- ExrxDocument3 pagesExrxapi-463720918No ratings yet
- Spirometry Interpretation: Lung VolumesDocument4 pagesSpirometry Interpretation: Lung VolumesBobet ReñaNo ratings yet
- Microsoft PowerPoint - BHDDocument35 pagesMicrosoft PowerPoint - BHDandarias kevinNo ratings yet
- Pathology Lec 7Document63 pagesPathology Lec 7ahmadNo ratings yet
- AASM Scoring Manual Version 2.4 Berry Et Al. 2017Document89 pagesAASM Scoring Manual Version 2.4 Berry Et Al. 2017Jorge Borrani100% (4)