You might also like
- Enuresia Bob FLawsDocument2 pagesEnuresia Bob FLawssofeli100% (1)
- Acupuncture Pulse Diagnosis and the Constitutional Conditional ParadigmFrom EverandAcupuncture Pulse Diagnosis and the Constitutional Conditional ParadigmNo ratings yet
- Japanese Wooden Hammer Acupuncture TechniqueDocument2 pagesJapanese Wooden Hammer Acupuncture Techniquejhonny100% (3)
- The Acupuncture Prescription:: A Holistic Approach to HealthFrom EverandThe Acupuncture Prescription:: A Holistic Approach to HealthNo ratings yet
- Abdominal PalpationDocument11 pagesAbdominal PalpationDoctora SantanaNo ratings yet
- TCM Imassager Instruction Manual 2011.6Document24 pagesTCM Imassager Instruction Manual 2011.6drfaizal100% (1)
- Menopausal Syndrome FootDocument0 pagesMenopausal Syndrome Footrasputin22100% (1)
- Cheng AcupunctureforWomenwithObesity PDFDocument13 pagesCheng AcupunctureforWomenwithObesity PDFAshari Fisio180% (1)
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument18 pagesWorld's Largest Science, Technology & Medicine Open Access Book PublisherAndik SH100% (1)
- ShoulderDocument8 pagesShoulderMichalNo ratings yet
- Case Review Prana GogiaDocument6 pagesCase Review Prana GogiapranajiNo ratings yet
- 08152011-Article 0 PDFDocument2 pages08152011-Article 0 PDFЕвгений ТополовскийNo ratings yet
- Diabetes Perspectives and TreatmentsDocument32 pagesDiabetes Perspectives and TreatmentsyellahfellahNo ratings yet
- 2-3 Hara Diagnosis 02102013 PDFDocument14 pages2-3 Hara Diagnosis 02102013 PDFHendrawan PratamaNo ratings yet
- Shanghan Lun: Zabing Lun (Simplified ChineseDocument2 pagesShanghan Lun: Zabing Lun (Simplified ChineseDoktormin106No ratings yet
- Classic Pulse DiagnosisDocument31 pagesClassic Pulse DiagnosisJayaRakMinimarketNo ratings yet
- Five Shu PointsDocument8 pagesFive Shu PointsMartin Ramos AlvaradoNo ratings yet
- Acupuncture For Memory LossDocument3 pagesAcupuncture For Memory Losspeter911xNo ratings yet
- Compilation Conditions + FormulasDocument2 pagesCompilation Conditions + Formulaspeter911x0% (1)
- H R C W: Erbs That Elieve Oughing AND HeezingDocument7 pagesH R C W: Erbs That Elieve Oughing AND HeezingEdison HlmNo ratings yet
- Mother Child Points Theory and ApplicationsDocument3 pagesMother Child Points Theory and ApplicationsChetna Kanchan BhagatNo ratings yet
- Jingjin Sara - 604 Final PaperDocument19 pagesJingjin Sara - 604 Final Paperapi-549590947No ratings yet
- Foot AcupunctureDocument0 pagesFoot Acupuncturerasputin22No ratings yet
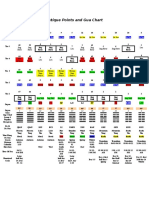
- Ancient Chinese Gua Chart and Organ PointsDocument1 pageAncient Chinese Gua Chart and Organ PointsPedro MaiaNo ratings yet
- TCM CatalogDocument16 pagesTCM CatalogNidhi RathodNo ratings yet
- 07 Caroline RadiceDocument7 pages07 Caroline Radicetigerstyle1No ratings yet
- Pulse Diagnosis Handouts 0Document9 pagesPulse Diagnosis Handouts 0ManviMittalNo ratings yet
- A Study of The Sa-Ahm Five Element Acupuncture Theory: December 2009Document13 pagesA Study of The Sa-Ahm Five Element Acupuncture Theory: December 2009dtncorreoNo ratings yet
- Acupuncture Treatment of AsthmaDocument20 pagesAcupuncture Treatment of AsthmafrankgzlNo ratings yet
- Alchemical Facial Acupuncture Protocols, Part 3: by Mary Elizabeth Wakefield, Lac, Dipl. Ac., MS, MMDocument3 pagesAlchemical Facial Acupuncture Protocols, Part 3: by Mary Elizabeth Wakefield, Lac, Dipl. Ac., MS, MMHaryono zhuNo ratings yet
- Alopecia areata: Hair loss disease explainedDocument0 pagesAlopecia areata: Hair loss disease explainedrasputin22100% (1)
- WirBel Seule PunkTeDocument1 pageWirBel Seule PunkTeRomi BrenerNo ratings yet
- Identifying Points Master TungDocument88 pagesIdentifying Points Master Tungangel 1958No ratings yet
- Scalp AcupunctureDocument1 pageScalp AcupunctureTaimoor DogarNo ratings yet
- FORMULAS FOR URINARY DIFFICULTY - Dr. Jake Fratkin - Boulder, CODocument5 pagesFORMULAS FOR URINARY DIFFICULTY - Dr. Jake Fratkin - Boulder, COVera Gardasevic MitrovicNo ratings yet
- TCM SampleDocument13 pagesTCM Sampleapi-3769511No ratings yet
- Two Acupuncture Styles for Painful Diabetic NeuropathyDocument7 pagesTwo Acupuncture Styles for Painful Diabetic NeuropathyAnonymous PFNzHoNo ratings yet
- TCM Healthier LivingDocument21 pagesTCM Healthier LivingToffler NiemuthNo ratings yet
- ScoliosisDocument9 pagesScoliosisexcalidorNo ratings yet
- Neoclassical Acupuncture and a Childhood CallingDocument13 pagesNeoclassical Acupuncture and a Childhood CallingzhikNo ratings yet
- Point Theory Final Study GuideDocument9 pagesPoint Theory Final Study GuidenoelleNo ratings yet
- Acupuncture For The Treatment of Chronic Painful Peripheral Diabetic Neuropathy: A Long-Term StudyDocument7 pagesAcupuncture For The Treatment of Chronic Painful Peripheral Diabetic Neuropathy: A Long-Term StudyFernanda GiulianoNo ratings yet
- 1996 Root and Branch Clinical ApplicationsDocument9 pages1996 Root and Branch Clinical Applicationsdoktormin106No ratings yet
- The Spark in The MachineDocument53 pagesThe Spark in The MachineElanghovan Arumugam100% (1)
- Diabetes MellitusDocument8 pagesDiabetes Mellitusab21423No ratings yet
- Summary of Chapter 11 of The Líng ShūDocument2 pagesSummary of Chapter 11 of The Líng ShūElanghovan ArumugamNo ratings yet
- Traditional Chinese MedicineDocument63 pagesTraditional Chinese MedicineTrisNo ratings yet
- Acupuncture Imaging 31 40 PDFDocument10 pagesAcupuncture Imaging 31 40 PDFmamun31No ratings yet
- AccupointDocument2 pagesAccupointDanuSusantoNo ratings yet
- M.E.a.D. Report ComparisonsDocument1 pageM.E.a.D. Report ComparisonsFaisal MadjidNo ratings yet
- Shonishin - AcupDocument2 pagesShonishin - AcupKoa Carlos CastroNo ratings yet
- Objectives: Traditional Chinese Acupuncture (TCM)Document7 pagesObjectives: Traditional Chinese Acupuncture (TCM)Anonymous lSZ9JVNo ratings yet
- Self-exam on eczema treatment patternsDocument4 pagesSelf-exam on eczema treatment patternsJiayiNo ratings yet
- Using Acupuncture Points To Eliminate Jet LagDocument5 pagesUsing Acupuncture Points To Eliminate Jet Lagsale18100% (1)
- Stabilize & Bind 1Document1 pageStabilize & Bind 1keirakuNo ratings yet
- Tugas Farmakologi ToksikologiDocument55 pagesTugas Farmakologi ToksikologilucyanaNo ratings yet
- Iron and CooperDocument1 pageIron and CooperDan AlexNo ratings yet
- SuJok TherapyDocument92 pagesSuJok Therapyspiritualbeing96% (25)
- Xogen - Tap Water As FuelDocument1 pageXogen - Tap Water As FuelDan AlexNo ratings yet
- Guasha 50 PatologiiDocument55 pagesGuasha 50 PatologiiDan Alex100% (2)
- Genetic Approach To Elucidation of Sasang Constitutional MedicineDocument7 pagesGenetic Approach To Elucidation of Sasang Constitutional MedicineDan Alex100% (1)
- Michael Stanborough - Direct Release Myofascial Technique - An Illustrated Guide For PractitionersDocument185 pagesMichael Stanborough - Direct Release Myofascial Technique - An Illustrated Guide For PractitionersDan Alex89% (19)
- Acupuncture - ChakrasDocument5 pagesAcupuncture - Chakrasfedefusaro100% (1)
- A Study of The Sa-Ahm Five Element Acupuncture Theory: EducationDocument12 pagesA Study of The Sa-Ahm Five Element Acupuncture Theory: EducationDan AlexNo ratings yet
- Crazy for the Storm: A Memoir of SurvivalFrom EverandCrazy for the Storm: A Memoir of SurvivalRating: 3.5 out of 5 stars3.5/5 (217)
- Becky Lynch: The Man: Not Your Average Average GirlFrom EverandBecky Lynch: The Man: Not Your Average Average GirlRating: 4.5 out of 5 stars4.5/5 (12)
- Horse Training 101: Key Techniques for Every Horse OwnerFrom EverandHorse Training 101: Key Techniques for Every Horse OwnerRating: 4.5 out of 5 stars4.5/5 (27)
- Bloodlines: The True Story of a Drug Cartel, the FBI, and the Battle for a Horse-Racing DynastyFrom EverandBloodlines: The True Story of a Drug Cartel, the FBI, and the Battle for a Horse-Racing DynastyRating: 4 out of 5 stars4/5 (8)
- Elevate and Dominate: 21 Ways to Win On and Off the FieldFrom EverandElevate and Dominate: 21 Ways to Win On and Off the FieldRating: 5 out of 5 stars5/5 (4)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- Endure: How to Work Hard, Outlast, and Keep HammeringFrom EverandEndure: How to Work Hard, Outlast, and Keep HammeringRating: 4.5 out of 5 stars4.5/5 (283)
- The Inside Game: Bad Calls, Strange Moves, and What Baseball Behavior Teaches Us About OurselvesFrom EverandThe Inside Game: Bad Calls, Strange Moves, and What Baseball Behavior Teaches Us About OurselvesRating: 4 out of 5 stars4/5 (7)
- I Never Had It Made: An AutobiographyFrom EverandI Never Had It Made: An AutobiographyRating: 3.5 out of 5 stars3.5/5 (38)
- The Teen’s Living Guide: Unlocking Your Potential for a Remarkable JourneyFrom EverandThe Teen’s Living Guide: Unlocking Your Potential for a Remarkable JourneyRating: 5 out of 5 stars5/5 (76)
- House of Nails: A Memoir of Life on the EdgeFrom EverandHouse of Nails: A Memoir of Life on the EdgeRating: 3 out of 5 stars3/5 (4)
- Badasses: The Legend of Snake, Foo, Dr. Death, and John Madden's Oakland RaidersFrom EverandBadasses: The Legend of Snake, Foo, Dr. Death, and John Madden's Oakland RaidersRating: 4 out of 5 stars4/5 (15)
- The Truth About Aaron: My Journey to Understand My BrotherFrom EverandThe Truth About Aaron: My Journey to Understand My BrotherNo ratings yet
- Patriot Reign: Bill Belichick, the Coaches, and the Players Who Built a ChampionFrom EverandPatriot Reign: Bill Belichick, the Coaches, and the Players Who Built a ChampionRating: 3.5 out of 5 stars3.5/5 (30)
- The Last Dive: A Father and Son's Fatal Descent into the Ocean's DepthsFrom EverandThe Last Dive: A Father and Son's Fatal Descent into the Ocean's DepthsNo ratings yet
- The Perfect Mile: Three Athletes, One Goal, and Less Than Four Minutes to Achieve ItFrom EverandThe Perfect Mile: Three Athletes, One Goal, and Less Than Four Minutes to Achieve ItNo ratings yet
- What Winners Won't Tell You: Lessons from a Legendary DefenderFrom EverandWhat Winners Won't Tell You: Lessons from a Legendary DefenderRating: 4.5 out of 5 stars4.5/5 (7)
- How Bad Do You Want It?: Mastering the Pshchology of Mind over MuscleFrom EverandHow Bad Do You Want It?: Mastering the Pshchology of Mind over MuscleRating: 4.5 out of 5 stars4.5/5 (127)
- Last Child in the Woods: Saving Our Children From Nature-Deficit DisorderFrom EverandLast Child in the Woods: Saving Our Children From Nature-Deficit DisorderRating: 4 out of 5 stars4/5 (283)
- The Mindful Athlete: Secrets to Pure PerformanceFrom EverandThe Mindful Athlete: Secrets to Pure PerformanceRating: 4.5 out of 5 stars4.5/5 (278)
- The Boys of Summer: The Classic Narrative of Growing Up Within Shouting Distance of Ebbets Field, Covering the Jackie Robinson Dodgers, and What's Happened to Everybody SinceFrom EverandThe Boys of Summer: The Classic Narrative of Growing Up Within Shouting Distance of Ebbets Field, Covering the Jackie Robinson Dodgers, and What's Happened to Everybody SinceRating: 4.5 out of 5 stars4.5/5 (18)